
“What’s your leadership style Cliff? How do you like to run the emergency department?”
Our new fellow had asked a reasonable question. Although I’d never had to summarise it before, my reply came immediately: “I see my role as doing the most for the most by reducing the sum total of human suffering in the ED – both patients and staff”.
I hadn’t really reflected on this before. Obviously my clinical priority is resuscitation, but the reality is that resuscitation only contributes to a small proportion of ED workload. And when our resources and attention are prioritised to the resus room, the department fills with other patients in pain or distress, and their anxious relatives and parents(1).
Examples of the suffering, in patients, relatives, and staff, include:
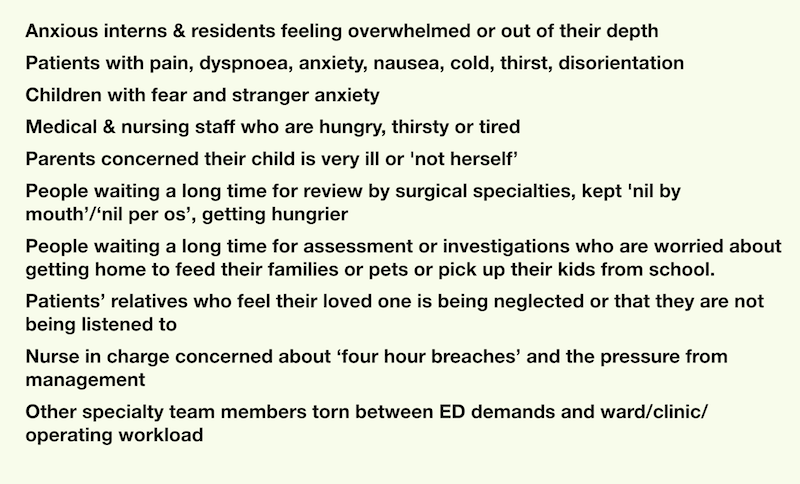
Emergency departments really can be melting pots of human suffering, but there is so much we can do to reduce or relieve that suffering.
We just need to expand our view of our role from ‘diagnose and treat illness’ to ‘care for patients and their families’.
I believe an emergency physician can do much to reduce the ‘area under the curve’ – from listening to the nurses, buying a round of coffee, making sure rest breaks happen; to relieving pain, thirst and cold; to trying to prevent illness and injury from claiming someone’s loved ones; to being understanding to an admitting specialty colleague; to taking the time to explain to parents and relatives what is going on, and that you are taking their presentation seriously.
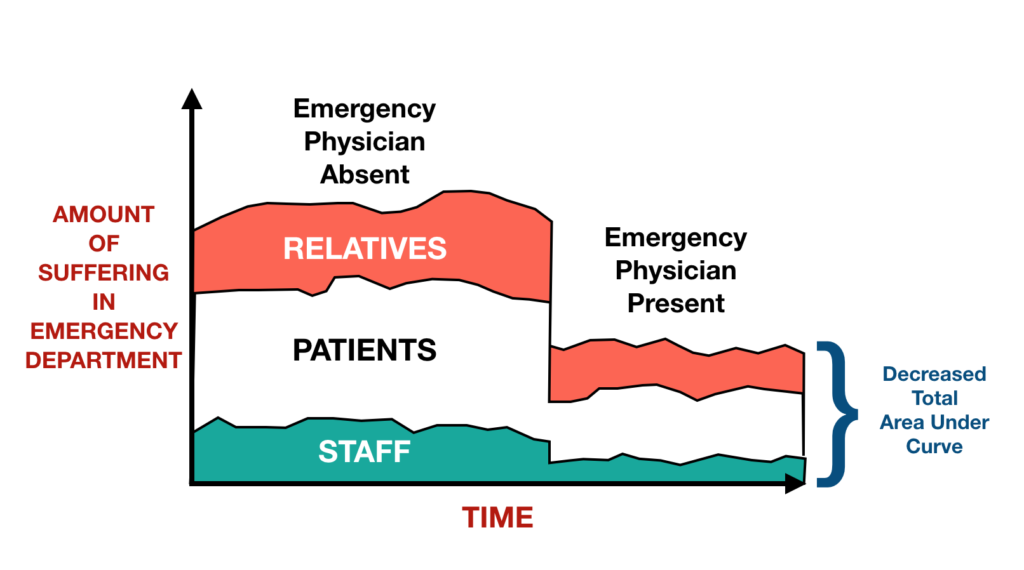
This is a graphic to illustrate a concept, not a graph based on data.
I also believe this approach provides some protection from burnout.
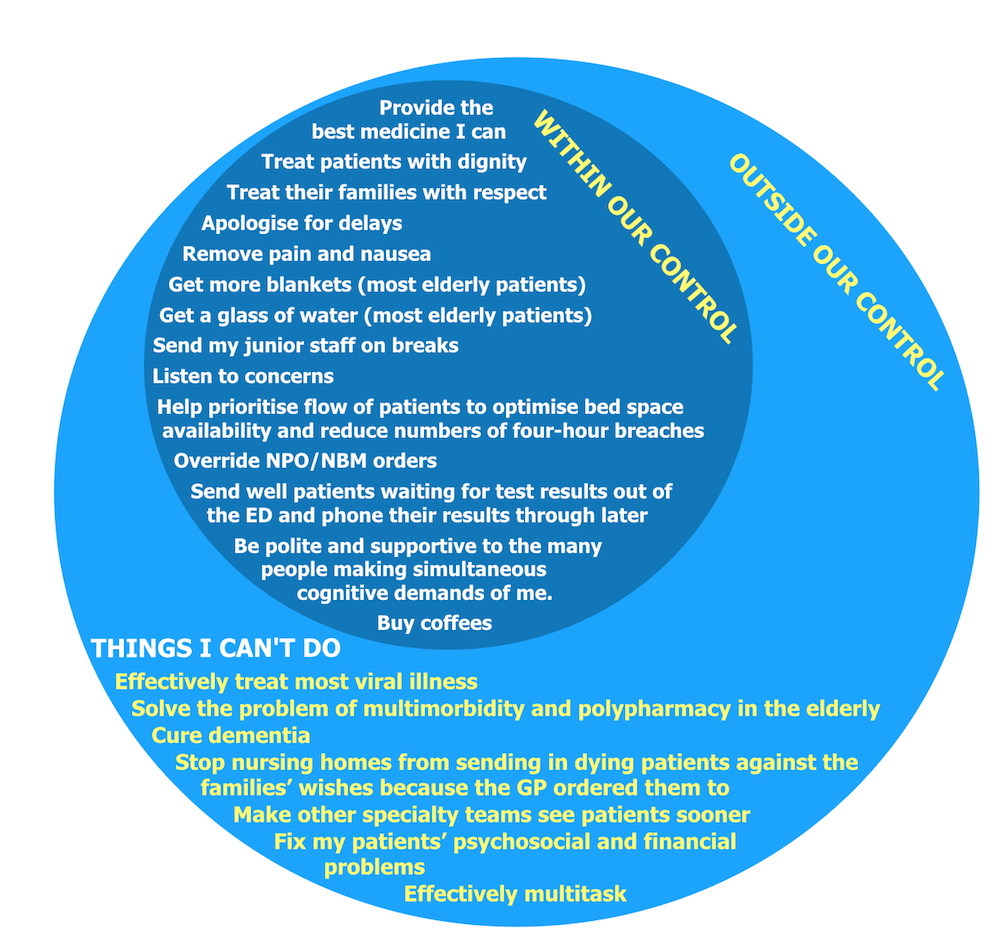
It is easy to be concerned with the difficult aspects of our job that are outside our control, which can result in stress and a sense of powerlessness. But there are so many things WITHIN our control that can make such a difference, that this is where our attention should focus.
This is the ‘Circle of Influence’ described by Steven Covey in “The 7 Habits of Highly Effective People”, in which he argues that the first habit, Proactivity, is demonstrated by people who work on problems within their circle of influence, rather than wasting time on those things outside it. Not only will this provide us with more satisfaction and sustainability in our career, it should also make us happier people, since expressing kindness for other people is a key component in the recipe for human happiness (which I describe here).
Of course, the other staff can also make a massive difference. However as the emergency physician clinically in charge of the floor, I have a responsibility to lead by example, and can exert far greater influence than more junior staff. As summarised recently by Liz Crowe and colleagues(2):
“EM doctors as the leads of the ED often set the ‘tone’ for the interdisciplinary staff within the team. Each EM doctor can choose to actively contribute to building a safe and supportive culture of collegial
support, professional development and learning through high quality communication, humour and creating a sense of team within their departments.”
So let’s ALL set the tone. Support our teams, and show kindness to them and our patients. We can all help reduce the Area Under the Suffering Curve.
1. Body R, Kaide E, Kendal S, Foëx B. Not all suffering is pain: sources of patients’ suffering in the emergency department call for improvements in communication from practitioners. Emerg Med J. 2015 Jan;32(1):15–20.
2. Crowe L, Young J, Turner J. The key to resilient individuals is to build resilient and adaptive systems. Emerg Med J. 2017 Jun 26;34(7):428–9.