This video shows the mechanism for dislodgement and deformation of humeral intraosseous needles and how to avoid this.
In summary, if you need to abduct the arm (eg. for thoracostomy), keep the thumbs down (ie. have the arm internally rotated at the shoulder). Otherwise the IO catheter may bend or fall out.
Occasionally we step out of the resuscitation room feeling like a case should have gone better, but it can be hard to put our finger on just where it went wrong. In my last post I discussed the STEPS approach to analysing resuscitation cases: Self, Team, Environment, Patient and System.
Occasionally you can get a case where the STEPS seem to be aligned but things still feel bad. In which the outcome was unsatisfactory because the plan was wrong, or the team wasn’t able to execute the plan. Consider the following case.
1. A patient with a past history of DVT no longer on anticoagulants presents with chest pain and syncope.
She is severely hypotensive with a raised jugular venous pressure and a clear chest x-ray. A working diagnosis of pulmomary embolism is made.
Discussions ensue regarding empirical fibrinolysis and a respiratory physician is consulted, who over the phone cautions against treating without a CT pulmonary angiogram.
The patient is given heparin and transferred to the CT scanner where she arrests. Intravenous rtPA is given during CPR but no return of spontaneous circulation is achieved and she is pronounced dead after 30 minutes of resuscitation.
On this occasion the team worked efficiently and communicated well under clear leadership. Everyone knew the plan and shared the mental model. The environment was well controlled and the patient had been swiftly moved to CT within 20 minutes of arrival. Thanks to simulation training the well rehearsed cardiac arrest resuscitation was conducted with precision and the team was able to rapidly access the thrombolytic and knew the correct dose.
By a quick STEPS analysis, this case appears to have gone as well as could be expected. Perhaps there is nothing to learn. Some you win, some you lose, no?
No. Autopsy revealed type A aortic dissection with pericardial tamponade.
The management may have been efficient but it failed to be effective. In other words, things were done right, but the right things weren’t done; they did the wrong things right.
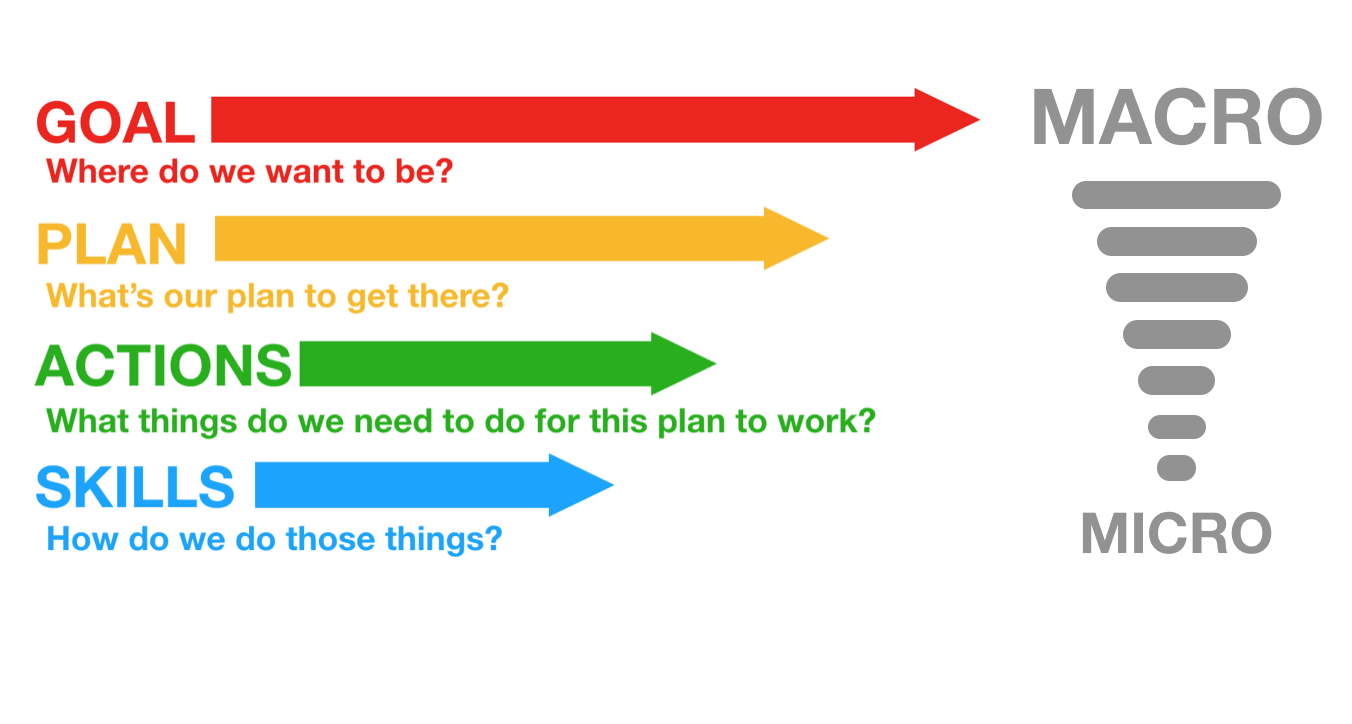
This might be an example where STEPS is inadequate, and instead we should evaluate the clinical trajectory. The cognitive bias that led to a lack of consideration of alternative diagnoses might be classifiable under ‘self’ or ‘team’ but I find it more helpful to consider it under a failure of strategy. What is strategy? Strategy in my mind is another word for plan. The plan is based on a particular resuscitation goal, and will consist of the procedures & skills required to action the plan. We can thus break down an attempted clinical trajectory into:
Goal (what are we trying to achieve) Strategy, or Plan (what’s our plan to get there?) Tactics, or Actions (what procedures will be required to execute the plan) And, at more granular level: If we’re failing at the procedural level, the components of procedures, namely Skills & Microskills. So, as we zoom in from macro to micro in setting the clinical trajectory, we can look at Goals, Plan, Actions, and Skills: In the above case it appears the following was applied, in terms of Goal-Plan-Actions-Skills:
G – resuscitate hypotensive patient P – give fibrinolysis for likely PE A – consult respiratory physician, get CTPA S – request scan, give heparin, transport to CT
The goal was appropriate, but the plan was ineffective.
The following approach would have been more effective.
G – resuscitate hypotensive patient P – identify cause of undifferentiated hypotension and initiate treatment in the resus room A – thorough bedside assessment in patient too sick to move: history, physical, CXR, ECG, labs, POCUS S – Basic cardiac ultrasound
By planning to identify and treat the cause of hypotension in the resus room, the more appropriate investigation would have been selected (cardiac ultrasound) and the correct diagnosis is much more likely to have been made.
Let’s look at some other cases:
2. An 88-year-old male presents by ambulance to the ED with dizziness. He is hypotensive, pyrexial, hypoxic and confused.
His chest x-ray shows likely bronchopneumonia. He has appropriate initial resuscitation and ICU is consulted. Soon he is intubated and on high dose vasoactive medication with escalating doses despite ongoing hypotension, anuria, and a lactate of 11 mmol/l, increased from 8 on arrival.
As he is being wheeled off down the corridor towards ICU his distraught and frail wife arrives. She is taken to the quiet room where she explains that her husband would never want to be ‘on a life support machine’ and asks ‘can’t you just keep him comfortable’?
G – the goal – to provide maximally aggressive resuscitation – was not in keeping with the patient’s wishes. If the goal had been to provide care in accordance with his wishes, the plan could have included attempts to ascertain these sooner while providing initial treatment. Upon gaining sufficient information, a new goal can be established: maximising the patient’s comfort and dignity.
3. An obese 30-year-old female presents with syncope. At triage she is pale, tachycardic & hypotensive. Clinical and sonographic assessment, including free intraperitoneal fluid and a positive urine HCG, is suggestive of ruptured ectopic pregnancy.
The gynaecologist and anaesthetist ask the ED team to bring the patient straight to the operating room. The ED team spends 20 minutes struggling to obtain intravenous access, eventually placing a 22G intravenous catheter in the patient’s hand and a humeral intraosseous needle.
Her shock is considerably worse on arrival in theatre, despite attempts to transfuse O negative blood en route.
Goal – get her safely to the operating room Plan – vascular access, cross match blood, start haemostatic resuscitation, go to OR as soon as possible Actions – peripheral and/or intraosseous cannulation attempts Skills – vascular access skills
Here the failure was at the actions and skills level. Better vascular access could have been attained using ultrasound guided peripheral cannulation, or central vascular access, or earlier intraosseous insertion.
4. A 120kg 32-year-old male with a history of deliberate self harm presents on the night shift with coma due to mixed benzodiazepine and venlafaxine overdose.
The decision is made to intubate for airway protection. After rapid sequence induction direct laryngoscopy is attempted by the emergency registrar who obtains a grade 4 view. Cricoid pressure is removed resulting in a grade 3 view.
The registrar asks for a bougie which she passes and then railroads the tracheal tube over it. The cuff is inflated, capnography is connected, and the self-inflating bag is connected and squeezed while the chest is auscultated.
The abdomen distends, the capnograph remains flat, and gastric contents are seen to pass upward through the tube into the self-inflating bag. The tube is immediately removed and bag-mask ventilation is attempted. The oxygen saturation is now 78% and the airway is soiled. The airway is suctioned and repeat attempts to bag-mask ventilate fail. A successful cricothyroidotomy is performed and the patient subsequent has full neurological recovery.
Goal – Provide supportive care and minimise complications from overdose Plan – Airway protection and admit to ICU for monitoring Actions – Rapid sequence intubation, ICU referral Skills – Pre-, peri- and post-intubation oxygenation techniques; patient positioning; rapid sequence induction of anaesthesia; direct laryngoscopy; bougie handling techniques; external laryngeal manipulation
In this case the patient was not placed in the ramped position and no nasal cannulae were applied for apnoeic oxygenation. A tube was railroaded over an oesophageal bougie, which arguably should not occur if ‘hold up’ is sought when the bougie is placed.
Although the goal, plan and actions were appropriate, the team did not demonstrate adequate skill in this procedure. Likely due to a failure of training, standardised procedures, and checklists (or their application), this could also be identified as a ‘system’ problem in STEPS. It is also possible that the intubator forgot her training under stress – a problem classifiable under ‘self’. Alternatively other members of the team may have had knowledge but didn’t speak up or cross-check their colleague, which would be a ‘team’ issue.
Limitations of this approach This sort of analysis is retrospective and subjective and at risk of hindsight bias (e.g. distortion due to projection, denial, or selective recall). However, these limitations do not negate the value of the learning exercise, particularly if we are aware of them and strive to minimise their impact (e.g. write down the details of a cases as soon as possible afterward). It at least provides a structure for individuals and teams to begin the conversation about where and how things may have been suboptimal.
Goals may be multiple and may change according to incoming information, and for each goal there may be several viable alternative plans. STEPS and GPAS may overlap, eg. team failures may result in inappropriate goals and strategies, or in failed procedures.
Summary These models may prove helpful as a means of dissecting a case in a structured way. Put simply, STEPS offers a structure for identifying efficiency improvements (“doing things right”) and GPAS can help us assess effectiveness (“doing the right things”).
Another way of looking at it is that STEPS provides the components of a resus at any point in time, and GPAS defines the trajectory: where the resus is going and how to get there.
I use this structure to analyse cases in my own clinical practice and in my teaching. I would be interested to hear from others’ experience. Do you find this approach useful in identifying areas for improvement in those cases that you feel should have gone better?
Thanks to Chris Nickson for his comments and improvements to this post
A resuscitationist agonises. These words, expressed by Scott Weingart during a podcast we did together, ring true to all of us who strive to improve our practice. Driven by the passionate conviction that we should never lose a salvageable patient through imperfect care, we relive cases and re-run them through our mental simulators to identify areas for improvement.
In the search for actionable items though, we occasionally exit this process empty-handed. Something about a case felt wrong although ostensibly all the clinical interventions may have been appropriate. It is in these cases that it can be helpful to have a structure to aid analysis.
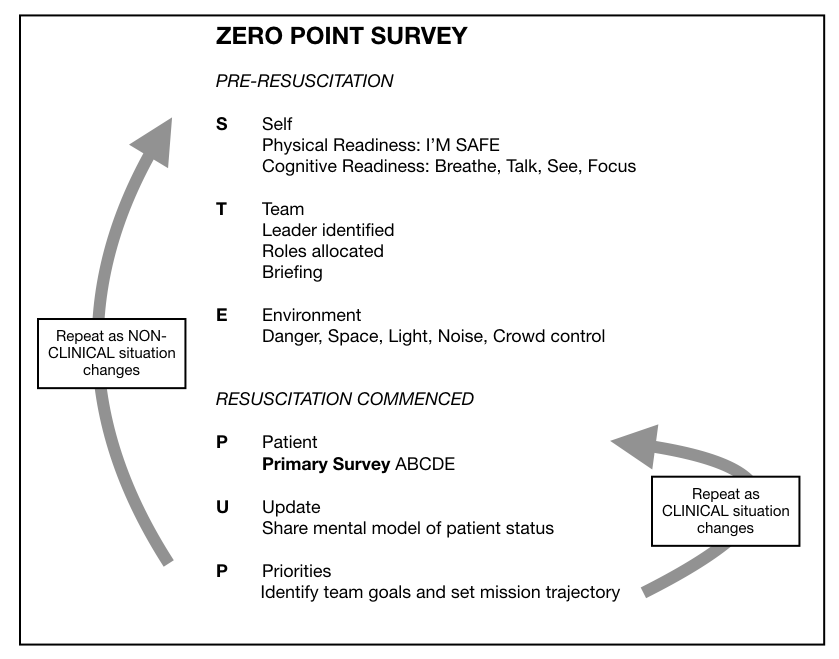
I, along with an international, interdisciplinary faculty of resuscitationists, have previously proposed an easily remembered system for optimising the clinical and non-technical components of resuscitation immediately before and during a patient encounter, dubbed the ‘Zero Point Survey’ (ZPS)(1), so called because first contact with a patient is rarely ‘Time Zero’ for a prehospital mission or hospital resuscitation case; there is invariably time for preparation of oneself, one’s team, and the environment (including equipment) prior to the primary survey and commencement of resuscitation. Following the assessment and management of STEP (self, team, environment & patient), the team should be regularly Updated on patient status and informed of the Priorities.
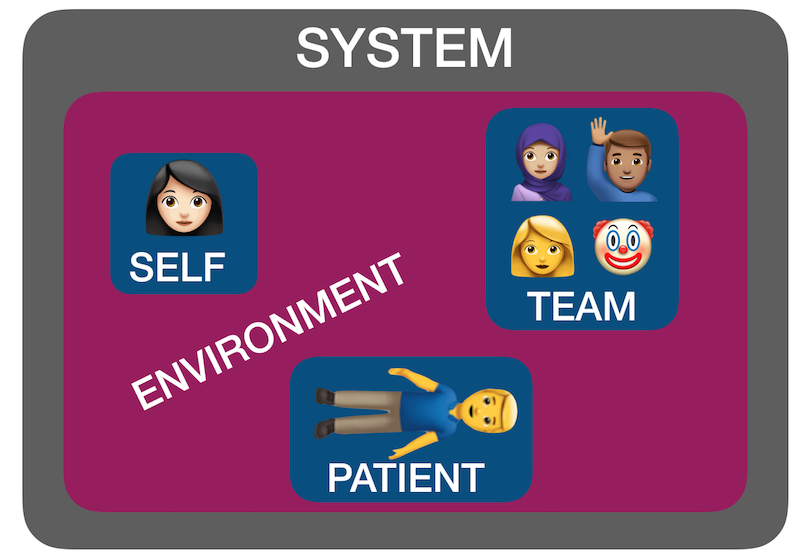
But ‘self, team, environment and patient’ isn’t just a useful system for case preparation. It can also be used for case analysis. I have found by discussing many ‘unsatisfactory’ cases over the years with participants in human factors workshops that STEP can help us identify where the issues lie. Accompanying all these factors is another ’S’: the system in which they interplay – the organisational rules, processes, policies, resources and deficiencies that may facilitate or obstruct an effective resuscitation(2).
Using STEPS to analyse cases The following (genuinely) hypothetical resus cases demonstrate how the application of this framework – Self, Team, Environment, Patient, System – might help identify correctible factors for future resuscitations:
1. Cardiac arrest in the bathroom on the orthopaedic ward – “it was chaos, there were too many people, and the resus trolley wasn’t properly stocked”.
STEPS analysis: Team – Leader needed to assign roles and allocate tasks Environment – Crowd control needed, lack of equipment System – Adequate checks for resus trolley not in place
2. 19-year-old male stabbed in the chest and arrested on arrival in hospital. CPR provided but went from PEA to asystole. Team leader discontinued resus after 20 minutes. Resident: “I thought he needed a resuscitative thoracotomy but no-one was willing to do it. No-one even mentioned it”.
STEPS analysis: Self – Lacked confidence to speak up, doubted own knowledge or influence Team – Lack of team situational awareness or knowledge or skill regarding required intervention System – Insufficient training and preparation for penetrating traumatic cardiac arrest scenario
3. 30-year-old mother with abdominal wound and her 2-year-old daughter with massive open head injury, both due to gunshot wounds, having been shot by husband/father who killed himself on scene. Child arrests in the ED, without ROSC, witnessed by mother before mother is taken to operating theatre.
STEPS analysis: Patient(s) – tragic case with upsetting circumstances and compounded psychological distress for patient and staff. The best resuscitation team in the world is not going to feel good about this one.
4. 46-year-old previously healthy male with VF arrest achieved ROSC after prehospital defibrillation and brought to the ED of a non-cardiac centre comatose and intubated. Further refractory VF in ED. Received multiple shocks, antiarrhythmics, double sequential external defibrillation. No on-site access to mechanical CPR, cardiac catheterisation, or ECMO. Patient declared dead in ED.
STEPS analysis: System – Prehospital team gave excellent care but brought the patient to a hospital ill-equipped to manage his ongoing needs, due to lack of ambulance service policy regarding appropriate destination hospital for cardiac arrest cases.
Summary You can see from the above cases how STEPS may be applied to make some sense of where a resus has gone wrong. Note that I am not recommending this as a way of structuring a team debrief or formal incident investigation – many institutions already have processes for conducting these and various rules and sensitivities have to be accommodated. Rather, this is a format I’ve found helpful in applying during informal discussions that aim to get the nub of where things could or should have gone better.
Occasionally, you can get a case where the STEPS seem to be aligned but things still feel bad – in which the outcome was unsatisfactory because the plan was wrong, or the team wasn’t able to execute the plan. In my next post I’ll discuss another way of analysing cases that can accompany STEPS.
An engaging scene from ‘Code Blue‘ demonstrated a Helicopter Emergency Medical Service team managing a patient with major thoracic haemorrhage. They did a right thoracotomy and wanted to clamp the hilum but there was some kit missing from the pack.
Unfortunately, the video is no longer available.
This scene had some great discussion points for prehospital professionals, even if the specific scenario is somewhat unlikely for most people’s practice:
Non-compressible haemorrhage is possibly the biggest single clinical challenge when you’re a long way from hospital
Agitated friends and family can be disruptive – allocate a rescuer to look after them
Having blood products to give is essential
Don’t rely on the memory of individuals, who are fallible, to pack your equipment. “I was sure I put them in” didn’t cut it when the team needed forceps to clamp the pulmonary hilum and stop the bleeding. Checklists are the in thing, for good reason.
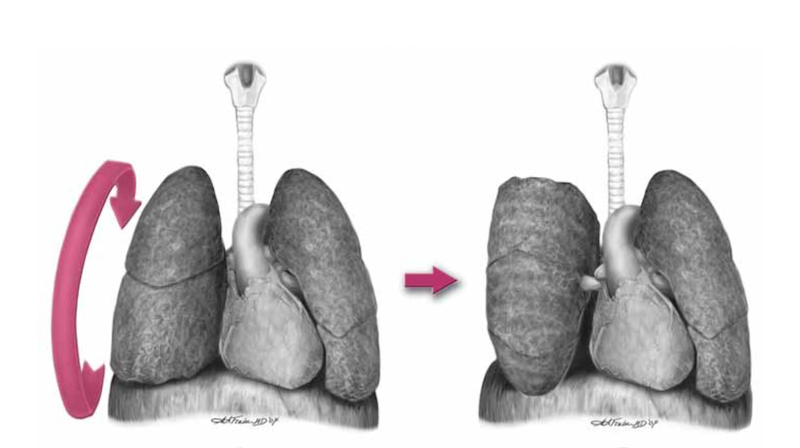
Luckily, you don’t need to clamp the hilum (which is tricky) in massive unilateral thoracic haemorrhage. You can just twist the lung 180 degrees on the hilum so it’s upside down. This can prevent further haemorrhage and air embolism.
What’s a hilar twist then?
The hilar twist manoeuvre, as it’s called, is worth learning if you’re a clinician who is prepared to do resuscitative clamshell thoracotomy for penetrating traumatic cardiac arrest. The clamshell is quick and provides excellent exposure(1) and is preferred to lateral thoracotomy(2).
The primary purpose of clamshell thoracotomy in penetrating traumatic arrest is to relieve cardiac tamponade and control a cardiac wound(3). It is well described and continues to save lives in the prehospital setting(4).
However, sometimes you’ll open the chest and the pericardium will be empty (other than containing the heart of course), and there will be massive haemorrhage on one side of the chest. Although most of these patients will be unsalvageable outside a trauma centre’s operating room, it’s worth trying something once you’ve gone to all the trouble of opening the chest. The hilar twist(5) is probably the best option for the non-surgeon, especially when some muppet’s forgotten to pack a clamp.
In order to make the lung mobile enough to twist, it’s first necessary to cut through the inferior pulmonary ligament. This is also known as simply the pulmonary ligament (because there’s no superior equivalent) and sometimes the inferior hilar ligament. It’s not actually a ligament, but an extension of the parietal pleura extending downwards in a fold from the hilum. Some describe it as hanging down from the hilum like a ‘wizard’s sleeve’, which invariably gets a giggle from some of our trainees from the United Kingdom for some reason.
After cutting the ligament completely to the level of the inferior pulmonary vein, the lung is then twisted ‘lower lobe towards you’, ie. lower lobe is rotated anteriorly over the upper lobe until the lung is oriented ‘upside down’. The twisted vessels around the hilum become occluded and further haemorrhage from that side should be limited. Other priorities in the arrested patient will be aortic occlusion, internal cardiac massage, and blood products. Packs may be required to keep the lung from untwisting, and if return of spontaneous circulation is achieved, there is a risk of dysrhythmia, right heart failure, and refractory hypoxaemia.
I’ve only done this on pigs and human cadavers so am not speaking from any reassuring level of experience or competence. The literature is out there to read, and it’s up to you to decide how you want to expand or limit your options when you’ve cracked that chest in an arrested patient.
References
1. Flaris AN, Simms ER, Prat N, Reynard F, Caillot J-L, Voiglio EJ. Clamshell incision versus left anterolateral thoracotomy. Which one is faster when performing a resuscitative thoracotomy? The tortoise and the hare revisited. World J Surg. 2015 May;39(5):1306–11.
2. Simms ER, Flaris AN, Franchino X, Thomas MS, Caillot J-L, Voiglio EJ. Bilateral Anterior Thoracotomy (Clamshell Incision) Is the Ideal Emergency Thoracotomy Incision: An Anatomic Study. World J Surg. 2013 Feb 23;37(6):1277–85.
The London Trauma Conference remains up there on my list of ‘must go’ conferences to attend. It marks the end of the year, fills me with hope and inspires me for the future. Unfortunately this year I was torn between the conference and the demands of clinical directorship so I could only get to the “Air Ambulance & Prehospital Care Day”. At least this way I’m saved from the dilemma of which sessions to attend!
So what were the highlights of the Prehospital Day? For me, they were Prehospital ECMO,’Picking Up the Pieces’, and the REBOA update. Prehospital ECMO Professor Pierre Carli gave us an update on prehospital ECMO. Professor Carli (not to be confused with the equally awesome Professor Carley) is the medical director of Service d’Aide Médicale Urgente (SAMU) in Paris. They’ve been doing prehospital ECMO in Paris since 2011 and the data analysed over three years reveals a 10% survival to hospital discharge rate. We know from the work in Asia that successful outcome following traditional cardiac arrest management and ECPR is related to the speed of the intervention. Transposing the time to intervention from his 2011 – 2013 data onto the survival curve that Chen et al produced explains why the success rate is limited:
The revised 2015 process aims to reduce the duration of CPR, reduce time to ECMO and therefore improve survival to discharge rates. They are doing this by dispatching the ECMO team earlier.
The eligibility criteria for ECPR is also changing; patients >18 and <75years, refractory cardiac arrest (defined as failure of ROSC after 20min of CPR), no flow for < 5 minutes with shockable rhythm or signs of life or hypothermia or intoxication, EtCO2 > 10mmHg at time of inclusion and no major comorbidity.
Already there appears to be an improvement with 16 patients treated using the revised protocol with 5 survivors (31%) – although we must be wary of the small numbers.
A concern that was expressed by the French Department of Health was the fear of a reduction in organ donation with the introduction of ECPR – it turns out that rates have remained stable. In fact the condition of non heart beating donated organs is better when ECMO has been instigated; the long term effects on organ donation are being assessed.
I’m without doubt that prehospital ECMO/ED ECMO is the future although currently in the UK our hospital systems aren’t ready for this. If you want to learn more then look at the ED ECMO site or book on one of the many emerging courses on ED ECMO including the one that is run by Dr Simon Finney at the London Trauma Conference, or if you want to go further afield you could try San Diego (although places are fully booked on the next course). Picking Up the Pieces
The Keynote speaker was Professor Sir Simon Wessely. He is a psychiatrist with a specialist interest in military psychology and his brief was to describe to us the public response to traumatic incidents. He has worked with the military and in civilian situations. After the 7/7 London bombings the population of London was surveyed: those most likely to be affected were of lower social class, of Muslim faith, those that had a relative that was injured, those unsure of the safety of others, those with no previous experience of terrorism and those experiencing difficulty in contacting others by mobile phone. Obviously there are many factors that we cannot influence however on the basis of the last risk factor our response to incidents has changed – the active discouragement to make phone calls has been changed to a recommendation of making short calls to friends and relatives.
The previous practice of offering immediate psychological debriefing to those involved in incidents was discounted by Prof Wessely – his research demonstrated that this intervention was not only not required but could actually result in harm: only a minority have ongoing psychological distress that can benefit from formal psychological input, which should occur later.
The approach that should be taken is to allow that individual to utilise their own social networks (family, friends, and colleagues) and to accept that in some cases the individual may not want or need to talk. This has led to the development of the Trauma Risk Management (TRIM) system which provides individuals within organisations that are exposed to traumatic events the skills required to identify those at risk of developing psychological problems and to recognise the signs and symptoms of those in difficulty. To a certain extent we naturally do this for our peers – I have spent many a night sitting in the ‘Good Samaritan’ pub with colleagues from the Royal London Hospital and London’s Air Ambulance – but having a more formal system is probably of benefit to enable those who have ongoing difficulties to access additional support. REBOA update
Finally, the REBOA update – Resuscitative Endovascular Balloon Occlusion of the Aorta. One year on, Dr Sammy Sadek informed us that there are now more courses teaching the REBOA technique than there are (prehospital) patients that have received it. Over the last year only seven patients have qualified for this intervention in London, far fewer than they had anticipated. Another three patients died before REBOA could be instigated. All patients had a positive cardiovascular response. Four of the seven died from causes other than exsanguination. Is it worth all the effort and resource to deliver this intervention when such a select group will benefit?
Obviously there was much more covered in the day, this is just a taste. If you’ve never been to the London Trauma Conference then I definitely would recommend it and even if you have been before there are so many breakout sessions now there is always something for everyone. More on the London Trauma Conference:
Keep an eye on the LTC website for information on the 2016 conference.
Thanks to Rob MacSweeney‘s fantastic Critical Care Reviews I learned of Idarucizumab, a monoclonal antibody fragment that binds the (pesky) anticoagulant dabigatran. Two industry-supported studies this week show rapid, complete reversal of anticoagulation in healthy volunteers(1) and patients who were either bleeding or undergoing procedures(2). The dose given to patients was 5g intravenously.
An accompanying editorial(3) highlights that the clinical study did not have a control group, and these patients had a high mortality. Further controlled studies examining patient-orientated outcomes will be helpful.
Of interest, another editorialist(4) lists other potential antidotes for Non-vitamin-K antagonist oral anticoagulants (NOACs) that have been or are being tested: an antidote against all oral direct factor Xa inhibitors called andexanet alpha (a recombinant activated factor X that binds direct factor Xa inhibitors), and a modified thrombin has been shown to be effective in vitro and in animals for reversal of dabigatran and potentially also other direct thrombin inhibitors.
1. Safety, tolerability, and efficacy of idarucizumab for the reversal of the anticoagulant effect of dabigatran in healthy male volunteers: a randomised, placebo-controlled, double-blind phase 1 trial The Lancet Volume 386, No. 9994, p680–690, 15 August 2015
[EXPAND Abstract]
BACKGROUND: Idarucizumab is a monoclonal antibody fragment that binds dabigatran with high affinity in a 1:1 molar ratio. We investigated the safety, tolerability, and efficacy of increasing doses of idarucizumab for the reversal of anticoagulant effects of dabigatran in a two-part phase 1 study (rising-dose assessment and dose-finding, proof-of-concept investigation). Here we present the results of the proof-of-concept part of the study.
METHODS: In this randomised, placebo-controlled, double-blind, proof-of-concept phase 1 study, we enrolled healthy volunteers (aged 18-45 years) with a body-mass index of 18·5-29·9 kg/m2 into one of four dose groups at SGS Life Sciences Clinical Research Services, Belgium. Participants were randomly assigned within groups in a 3:1 ratio to idarucizumab or placebo using a pseudorandom number generator and a supplied seed number. Participants and care providers were masked to treatment assignment. All participants received oral dabigatran etexilate 220 mg twice daily for 3 days and a final dose on day 4. Idarucizumab (1 g, 2 g, or 4 g 5-min infusion, or 5 g plus 2·5 g in two 5-min infusions given 1 h apart) was administered about 2 h after the final dabigatran etexilate dose. The primary endpoint was incidence of drug-related adverse events, analysed in all randomly assigned participants who received at least one dose of dabigatran etexilate. Reversal of diluted thrombin time (dTT), ecarin clotting time (ECT), activated partial thromboplastin time (aPTT), and thrombin time (TT) were secondary endpoints assessed by measuring the area under the effect curve from 2 h to 12 h (AUEC2-12) after dabigatran etexilate ingestion on days 3 and 4. This trial is registered with ClinicalTrials.gov, number NCT01688830.
FINDINGS: Between Feb 23, and Nov 29, 2013, 47 men completed this part of the study. 12 were enrolled into each of the 1 g, 2 g, or 5 g plus 2·5 g idarucizumab groups (nine to idarucizumab and three to placebo in each group), and 11 were enrolled into the 4 g idarucizumab group (eight to idarucizumab and three to placebo). Drug-related adverse events were all of mild intensity and reported in seven participants: one in the 1 g idarucizumab group (infusion site erythema and hot flushes), one in the 5 g plus 2·5 g idarucizumab group (epistaxis); one receiving placebo (infusion site haematoma), and four during dabigatran etexilate pretreatment (three haematuria and one epistaxis). Idarucizumab immediately and completely reversed dabigatran-induced anticoagulation in a dose-dependent manner; the mean ratio of day 4 AUEC2-12 to day 3 AUEC2-12 for dTT was 1·01 with placebo, 0·26 with 1 g idarucizumab (74% reduction), 0·06 with 2 g idarucizumab (94% reduction), 0·02 with 4 g idarucizumab (98% reduction), and 0·01 with 5 g plus 2·5 g idarucizumab (99% reduction). No serious or severe adverse events were reported, no adverse event led to discontinuation of treatment, and no clinically relevant difference in incidence of adverse events was noted between treatment groups.
INTERPRETATION: These phase 1 results show that idarucizumab was associated with immediate, complete, and sustained reversal of dabigatran-induced anticoagulation in healthy men, and was well tolerated with no unexpected or clinically relevant safety concerns, supporting further testing. Further clinical studies are in progress.
BACKGROUND: Specific reversal agents for non-vitamin K antagonist oral anticoagulants are lacking. Idarucizumab, an antibody fragment, was developed to reverse the anticoagulant effects of dabigatran.
METHODS: We undertook this prospective cohort study to determine the safety of 5 g of intravenous idarucizumab and its capacity to reverse the anticoagulant effects of dabigatran in patients who had serious bleeding (group A) or required an urgent procedure (group B). The primary end point was the maximum percentage reversal of the anticoagulant effect of dabigatran within 4 hours after the administration of idarucizumab, on the basis of the determination at a central laboratory of the dilute thrombin time or ecarin clotting time. A key secondary end point was the restoration of hemostasis.
RESULTS: This interim analysis included 90 patients who received idarucizumab (51 patients in group A and 39 in group B). Among 68 patients with an elevated dilute thrombin time and 81 with an elevated ecarin clotting time at baseline, the median maximum percentage reversal was 100% (95% confidence interval, 100 to 100). Idarucizumab normalized the test results in 88 to 98% of the patients, an effect that was evident within minutes. Concentrations of unbound dabigatran remained below 20 ng per milliliter at 24 hours in 79% of the patients. Among 35 patients in group A who could be assessed, hemostasis, as determined by local investigators, was restored at a median of 11.4 hours. Among 36 patients in group B who underwent a procedure, normal intraoperative hemostasis was reported in 33, and mildly or moderately abnormal hemostasis was reported in 2 patients and 1 patient, respectively. One thrombotic event occurred within 72 hours after idarucizumab administration in a patient in whom anticoagulants had not been reinitiated.
CONCLUSIONS: Idarucizumab completely reversed the anticoagulant effect of dabigatran within minutes. (Funded by Boehringer Ingelheim; RE-VERSE AD ClinicalTrials.gov number, NCT02104947.).
The focus of the entire day is cardiac arrest and this is the second day of the London Cardiac Arrest Symposium.
Professor Niklas Nielsen kicked off with a presentation of his Targeted Temperature Management trial. It seems that even now there is uncertainty in the interpretation of this latest study. I take heart from the knowledge that Prof Nielsen has changed the practice of his institution to reflect the findings of his study – I have certainly changed my practice. But we need to remain aware that there is more work to be done to answer the multiple questions that remain and the need for further RCTs is recognised.
The management of Cardiac arrest after avalanche is not a clinical scenario that I imagine I’ll ever find myself in. The management is well documented in the ICAR MEDCOM guidelines 2012. Dr Peter Paal reminded us that you’re not dead until you’re rewarmed and dead unless: with asystole, CPR may be terminated (or withheld) if a patient is lethally injured or completely frozen, the airway is blocked and duration of burial >35 min, serum potassium >12 mmol L(-1), risk to the rescuers is unacceptably high or a valid do-not-resuscitate order exists.
The age old question about prognostication after cardiac arrest was tackled by Prof Mauro Oddo. He covered the evidence for clinical examination, SSPE, EEG, and neurone specific enolase. Bottom line, all of these modalities are useful but none are specific enough to be used as a stand alone test so multiple modalities are required.
SAMU is leading the way with prehospital ECMO. They have mastered the art of cannulation (in the Louvre no less!) but there haven’t enough cases to demonstrate a mortality benefit. The commencement of ECMO prehospital reduces low flow time and theoretically should improve outcomes. This is begging for a RCT.
The experience of the Italians with in hospital ECMO shoes a better survival rate for in-hospital rather than out of hospital cardiac arrests, explained Dr Tomasso Mauri. They treat patients with a no flow time of <6min and low flow rate of <45min and had a 31% ICU survival rate. If you want to learn more about ED ECMO go to http://edecmo.org.
The Douglas Chamberlain lecture this year was Selective aortic arch perfusion presented by Prof James Manning. He spoke about the use of this technique in cardiac arrest and also in trauma (where it is known to you as Zone 1 REBOA).
In cardiac arrest the aim is to improve coronary perfusion, to preserve perfusion to the heart and the brain, offer a route of rapid temperature control and offer a direct route of administration of adrenaline. Coronary perfusion is seen to be supra normal after SAAP. And the suggested place for SAAP is prior to ECMO.
It’s more familiar ground talking about SAAP in trauma. This Zone 1 occlusion preserves cerebral and cardiac perfusion while blood loss is limited and rapid fluid resuscitation can occur.
You can hear Prof Manning on SAAP over at EMCrit (of course!).
It’s been another great conference. Put the dates for next year’s London Trauma & Cardiac Arrest Conferences in your diary: 8th-10th December 2015!
Day three is Air Ambulance and pre-hospital day and the great and the good are here en mass.
The heavy weights are coming out to make their points….. Unarguably the best lecture of the day was delivered by our very own Cliff Reid on prehospital training. Using Sydney HEMS induction training he highlighted the challenges posed to prehospital services training doctors and paramedics rotating through the service.
Turning a good inhospital doctor into a great prehospital one in the space of an induction program requires focus. Knowledge is therefore not the focus of training, performance is. Often doctors already possess the clinical skills and knowledge and it is the application of these pre existing skills in challenging environments when cognitively overloaded that is the key.
The Sydney HEMS program provides the mindware and communication skills the practitioner needs to do this and drills these skills in simulated environments. He uses perturbation, so like the Bruce protocol exercise test the simulations just get harder until you are at the very limits of your bandwidth. Debriefing of course is important but the recommended protracted debrief is often impractical and unnecessary so simulations designed with cognitive traps are used to highlight learning points and are drilled until the message is received. In this way tress exposure enhances cognitive resilience. And importantly they use cross training, so the doctors and the paramedics undergo the same program so each member of the team understands the challenges faced by the other.
Does this sound like fun? For the shrinking violets out there it could be seen as threatening. But for the adrenaline junkies…….hell yeah!
It’s truly a training ethos that I buy into and I’d love to be able to achieve that standard of training in my own service. Sydney HEMS Friends and Colleagues at the LTC
How would you transfer a psychotic patient requiring specialist intervention that can only be received after aeromedical transfer? Stefan Mazur of MedSTAR, the retrieval service in South Australia shared their experience with ketamine to facilitate the safe transfer of these patients with no reports of adverse effects on the mental state of the patient, as first described by Minh Le Cong and colleagues. Is there no end to the usefulness of this drug? No wonder we’re experiencing a supply issue in the UK!
And finally, the ultimate reflective practice should include the post mortem of our critically sick patients. The approach the forensic pathologist takes is similar to a clinician (with the time pressure removed). They read the scene and use this information to predict injuries (sound familiar?). Post mortem CT scanning with recon provides yet another layer of information. We are missing a trick if we don’t seek this feedback to correlate with our clinical findings. Even better, rare practical skills are often routinely performed as part of the post mortem – we should be making use of this opportunity to train.
I’ve travelled almost the entire length of England to get to the London Trauma Conference this year. What could be more important than attending one of the best conferences of the year? Examining for the DipRTM at the Royal College of Surgeons in Edinburgh
So was it worth the 4am start? Absolutely! My highlights would be Tom Evens explaining why trauma can be regarded like an elite sport. His background is as a sports coach in addition to his medical accomplishments and walking us through the journey he went through with the athlete he was coaching demonstrates the changes that need to occur when cultivating a performance culture and the results speak for themselves.
I can see similarities in the techniques used by athletes and those we are using in medicine now. Developing a highly performing team isn’t easy as anyone involved in the training of these teams will know.
Dr Jerry Nolan answered some questions about cervical spine movement in airway management. The most movement is seen in the upper cervical spine and there is no surprise that there is an increased incidence of cervical spine injury in unconscious patients (10%). The bottom line is that no movement clinicians will make of the cervical spine is greater than that at the time of injury. And whether it be basic airway manoeuvres, laryngoscopy or cricoid pressure the degree of movement is in the same ball park and unlikely to cause further injury. He states that he would use MILS like cricoid pressure and have a low threshold for releasing it if there are difficulties with the intubation. Of course many of us don’t use cricoid pressure in RSI anymore………..
After watching Tom and Jerry we heard that ATLS has had its day. Dr Matthew Wiles implores us to reserve ATLS for the inexperienced and move away from this outdated system and move to training in teams using local policies. The Cochrane reviewers found an increase in knowledge but no change in outcomes.
And finally Dr Deasy has convinced me that I will be replaced by a robot roaming around providing remote enhanced care. On the up side I might be the clinician providing that support.
More from me on this fantastic conference soon. In the meantime follow it on Twitter!









 Unarguably the best lecture of the day was delivered by our very own
Unarguably the best lecture of the day was delivered by our very own 
 Microwaves seem to be the future if diagnostic testing. This modality is fast, is associated with a radiation dose lower than that of a mobile phone, non invasive, portable and has been shown to provide good information. It can be used on heads for intracranial haemorrhage and stroke or chests for pneumothorax detection. It’s all in the early stages but seems like it will be a viable option in the future.
Microwaves seem to be the future if diagnostic testing. This modality is fast, is associated with a radiation dose lower than that of a mobile phone, non invasive, portable and has been shown to provide good information. It can be used on heads for intracranial haemorrhage and stroke or chests for pneumothorax detection. It’s all in the early stages but seems like it will be a viable option in the future. My highlights would be
My highlights would be  Dr Jerry Nolan answered some questions about cervical spine movement in airway management. The most movement is seen in the upper cervical spine and there is no surprise that there is an increased incidence of cervical spine injury in unconscious patients (10%). The bottom line is that no movement clinicians will make of the cervical spine is greater than that at the time of injury. And whether it be basic airway manoeuvres, laryngoscopy or cricoid pressure the degree of movement is in the same ball park and unlikely to cause further injury. He states that he would use MILS like cricoid pressure and have a low threshold for releasing it if there are difficulties with the intubation. Of course many of us don’t use cricoid pressure in RSI anymore………..
Dr Jerry Nolan answered some questions about cervical spine movement in airway management. The most movement is seen in the upper cervical spine and there is no surprise that there is an increased incidence of cervical spine injury in unconscious patients (10%). The bottom line is that no movement clinicians will make of the cervical spine is greater than that at the time of injury. And whether it be basic airway manoeuvres, laryngoscopy or cricoid pressure the degree of movement is in the same ball park and unlikely to cause further injury. He states that he would use MILS like cricoid pressure and have a low threshold for releasing it if there are difficulties with the intubation. Of course many of us don’t use cricoid pressure in RSI anymore………..