This is a one day run through of how I think every aspect of resuscitation and critical care in the emergency department should be done.
It combines my experience of more than twenty years as a specialist in emergency medicine, critical care, and retrieval medicine with the most up to date information from the latest literature.
The format is classroom case-based discussion, with key memorable concepts shared in a way that can make a lot of participants thing differently about the clinical stuff they see every day.
Yes, it’s impossible to cover everything in one day when the venue kicks us out at 5pm. But it is SO much fun trying. And we go to the pub after for anyone that wants to keep the conversation going.
Occasionally we step out of the resuscitation room feeling like a case should have gone better, but it can be hard to put our finger on just where it went wrong. In my last post I discussed the STEPS approach to analysing resuscitation cases: Self, Team, Environment, Patient and System.
Occasionally you can get a case where the STEPS seem to be aligned but things still feel bad. In which the outcome was unsatisfactory because the plan was wrong, or the team wasn’t able to execute the plan. Consider the following case.
1. A patient with a past history of DVT no longer on anticoagulants presents with chest pain and syncope.
She is severely hypotensive with a raised jugular venous pressure and a clear chest x-ray. A working diagnosis of pulmomary embolism is made.
Discussions ensue regarding empirical fibrinolysis and a respiratory physician is consulted, who over the phone cautions against treating without a CT pulmonary angiogram.
The patient is given heparin and transferred to the CT scanner where she arrests. Intravenous rtPA is given during CPR but no return of spontaneous circulation is achieved and she is pronounced dead after 30 minutes of resuscitation.
On this occasion the team worked efficiently and communicated well under clear leadership. Everyone knew the plan and shared the mental model. The environment was well controlled and the patient had been swiftly moved to CT within 20 minutes of arrival. Thanks to simulation training the well rehearsed cardiac arrest resuscitation was conducted with precision and the team was able to rapidly access the thrombolytic and knew the correct dose.
By a quick STEPS analysis, this case appears to have gone as well as could be expected. Perhaps there is nothing to learn. Some you win, some you lose, no?
No. Autopsy revealed type A aortic dissection with pericardial tamponade.
The management may have been efficient but it failed to be effective. In other words, things were done right, but the right things weren’t done; they did the wrong things right.
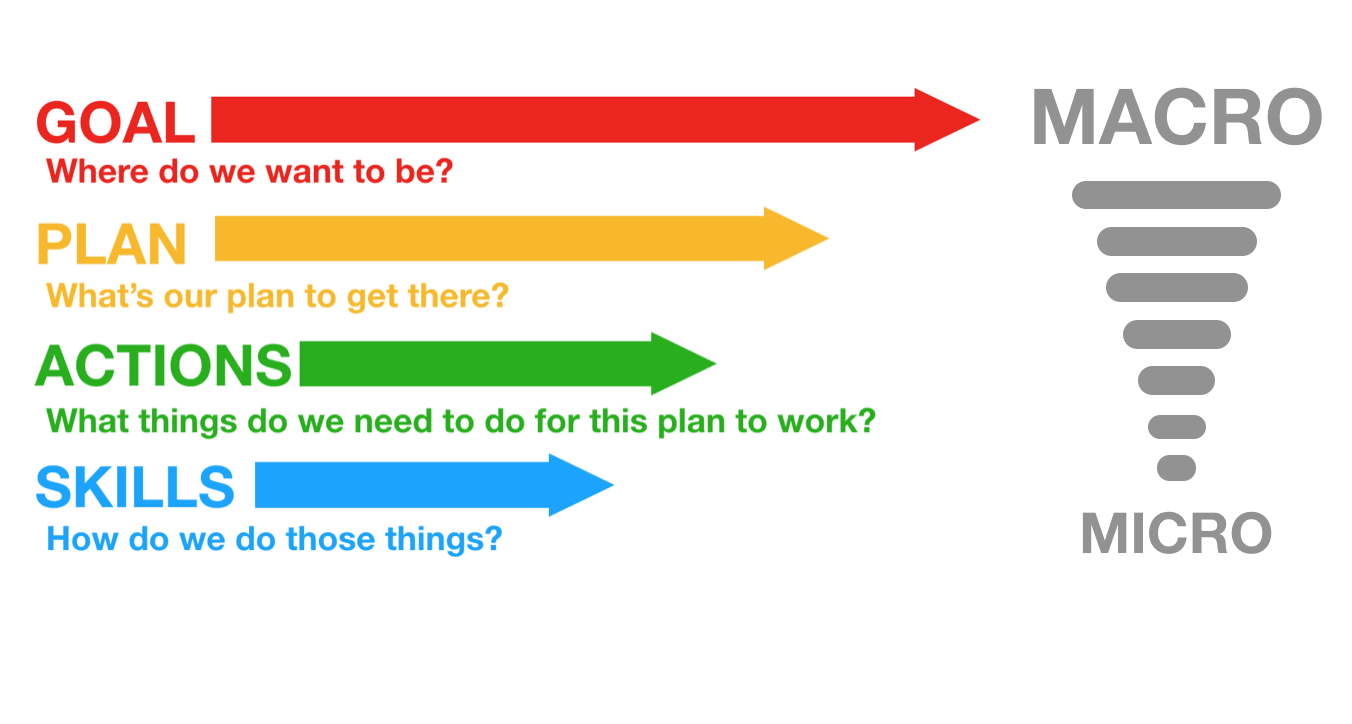
This might be an example where STEPS is inadequate, and instead we should evaluate the clinical trajectory. The cognitive bias that led to a lack of consideration of alternative diagnoses might be classifiable under ‘self’ or ‘team’ but I find it more helpful to consider it under a failure of strategy. What is strategy? Strategy in my mind is another word for plan. The plan is based on a particular resuscitation goal, and will consist of the procedures & skills required to action the plan. We can thus break down an attempted clinical trajectory into:
Goal (what are we trying to achieve) Strategy, or Plan (what’s our plan to get there?) Tactics, or Actions (what procedures will be required to execute the plan) And, at more granular level: If we’re failing at the procedural level, the components of procedures, namely Skills & Microskills. So, as we zoom in from macro to micro in setting the clinical trajectory, we can look at Goals, Plan, Actions, and Skills: In the above case it appears the following was applied, in terms of Goal-Plan-Actions-Skills:
G – resuscitate hypotensive patient P – give fibrinolysis for likely PE A – consult respiratory physician, get CTPA S – request scan, give heparin, transport to CT
The goal was appropriate, but the plan was ineffective.
The following approach would have been more effective.
G – resuscitate hypotensive patient P – identify cause of undifferentiated hypotension and initiate treatment in the resus room A – thorough bedside assessment in patient too sick to move: history, physical, CXR, ECG, labs, POCUS S – Basic cardiac ultrasound
By planning to identify and treat the cause of hypotension in the resus room, the more appropriate investigation would have been selected (cardiac ultrasound) and the correct diagnosis is much more likely to have been made.
Let’s look at some other cases:
2. An 88-year-old male presents by ambulance to the ED with dizziness. He is hypotensive, pyrexial, hypoxic and confused.
His chest x-ray shows likely bronchopneumonia. He has appropriate initial resuscitation and ICU is consulted. Soon he is intubated and on high dose vasoactive medication with escalating doses despite ongoing hypotension, anuria, and a lactate of 11 mmol/l, increased from 8 on arrival.
As he is being wheeled off down the corridor towards ICU his distraught and frail wife arrives. She is taken to the quiet room where she explains that her husband would never want to be ‘on a life support machine’ and asks ‘can’t you just keep him comfortable’?
G – the goal – to provide maximally aggressive resuscitation – was not in keeping with the patient’s wishes. If the goal had been to provide care in accordance with his wishes, the plan could have included attempts to ascertain these sooner while providing initial treatment. Upon gaining sufficient information, a new goal can be established: maximising the patient’s comfort and dignity.
3. An obese 30-year-old female presents with syncope. At triage she is pale, tachycardic & hypotensive. Clinical and sonographic assessment, including free intraperitoneal fluid and a positive urine HCG, is suggestive of ruptured ectopic pregnancy.
The gynaecologist and anaesthetist ask the ED team to bring the patient straight to the operating room. The ED team spends 20 minutes struggling to obtain intravenous access, eventually placing a 22G intravenous catheter in the patient’s hand and a humeral intraosseous needle.
Her shock is considerably worse on arrival in theatre, despite attempts to transfuse O negative blood en route.
Goal – get her safely to the operating room Plan – vascular access, cross match blood, start haemostatic resuscitation, go to OR as soon as possible Actions – peripheral and/or intraosseous cannulation attempts Skills – vascular access skills
Here the failure was at the actions and skills level. Better vascular access could have been attained using ultrasound guided peripheral cannulation, or central vascular access, or earlier intraosseous insertion.
4. A 120kg 32-year-old male with a history of deliberate self harm presents on the night shift with coma due to mixed benzodiazepine and venlafaxine overdose.
The decision is made to intubate for airway protection. After rapid sequence induction direct laryngoscopy is attempted by the emergency registrar who obtains a grade 4 view. Cricoid pressure is removed resulting in a grade 3 view.
The registrar asks for a bougie which she passes and then railroads the tracheal tube over it. The cuff is inflated, capnography is connected, and the self-inflating bag is connected and squeezed while the chest is auscultated.
The abdomen distends, the capnograph remains flat, and gastric contents are seen to pass upward through the tube into the self-inflating bag. The tube is immediately removed and bag-mask ventilation is attempted. The oxygen saturation is now 78% and the airway is soiled. The airway is suctioned and repeat attempts to bag-mask ventilate fail. A successful cricothyroidotomy is performed and the patient subsequent has full neurological recovery.
Goal – Provide supportive care and minimise complications from overdose Plan – Airway protection and admit to ICU for monitoring Actions – Rapid sequence intubation, ICU referral Skills – Pre-, peri- and post-intubation oxygenation techniques; patient positioning; rapid sequence induction of anaesthesia; direct laryngoscopy; bougie handling techniques; external laryngeal manipulation
In this case the patient was not placed in the ramped position and no nasal cannulae were applied for apnoeic oxygenation. A tube was railroaded over an oesophageal bougie, which arguably should not occur if ‘hold up’ is sought when the bougie is placed.
Although the goal, plan and actions were appropriate, the team did not demonstrate adequate skill in this procedure. Likely due to a failure of training, standardised procedures, and checklists (or their application), this could also be identified as a ‘system’ problem in STEPS. It is also possible that the intubator forgot her training under stress – a problem classifiable under ‘self’. Alternatively other members of the team may have had knowledge but didn’t speak up or cross-check their colleague, which would be a ‘team’ issue.
Limitations of this approach This sort of analysis is retrospective and subjective and at risk of hindsight bias (e.g. distortion due to projection, denial, or selective recall). However, these limitations do not negate the value of the learning exercise, particularly if we are aware of them and strive to minimise their impact (e.g. write down the details of a cases as soon as possible afterward). It at least provides a structure for individuals and teams to begin the conversation about where and how things may have been suboptimal.
Goals may be multiple and may change according to incoming information, and for each goal there may be several viable alternative plans. STEPS and GPAS may overlap, eg. team failures may result in inappropriate goals and strategies, or in failed procedures.
Summary These models may prove helpful as a means of dissecting a case in a structured way. Put simply, STEPS offers a structure for identifying efficiency improvements (“doing things right”) and GPAS can help us assess effectiveness (“doing the right things”).
Another way of looking at it is that STEPS provides the components of a resus at any point in time, and GPAS defines the trajectory: where the resus is going and how to get there.
I use this structure to analyse cases in my own clinical practice and in my teaching. I would be interested to hear from others’ experience. Do you find this approach useful in identifying areas for improvement in those cases that you feel should have gone better?
Thanks to Chris Nickson for his comments and improvements to this post
A resuscitationist agonises. These words, expressed by Scott Weingart during a podcast we did together, ring true to all of us who strive to improve our practice. Driven by the passionate conviction that we should never lose a salvageable patient through imperfect care, we relive cases and re-run them through our mental simulators to identify areas for improvement.
In the search for actionable items though, we occasionally exit this process empty-handed. Something about a case felt wrong although ostensibly all the clinical interventions may have been appropriate. It is in these cases that it can be helpful to have a structure to aid analysis.
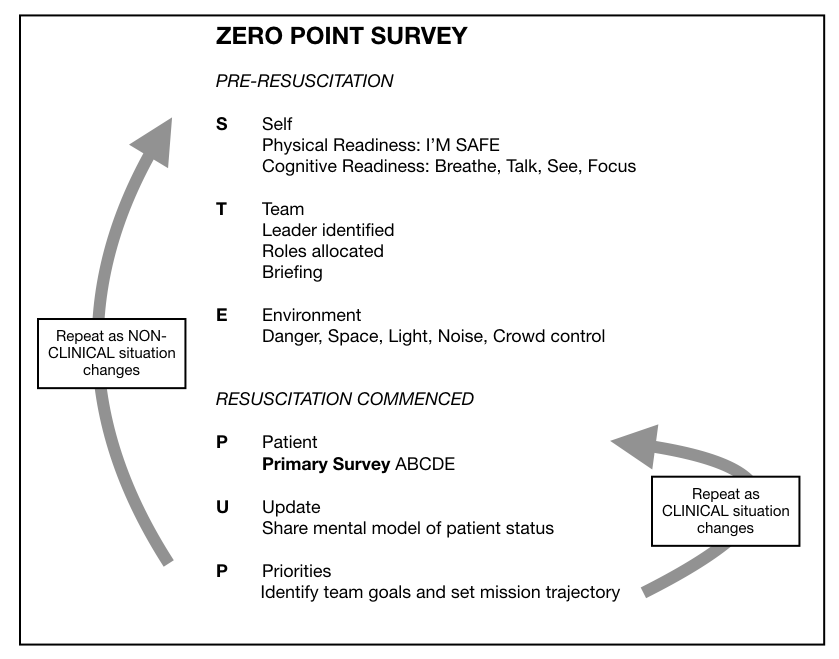
I, along with an international, interdisciplinary faculty of resuscitationists, have previously proposed an easily remembered system for optimising the clinical and non-technical components of resuscitation immediately before and during a patient encounter, dubbed the ‘Zero Point Survey’ (ZPS)(1), so called because first contact with a patient is rarely ‘Time Zero’ for a prehospital mission or hospital resuscitation case; there is invariably time for preparation of oneself, one’s team, and the environment (including equipment) prior to the primary survey and commencement of resuscitation. Following the assessment and management of STEP (self, team, environment & patient), the team should be regularly Updated on patient status and informed of the Priorities.
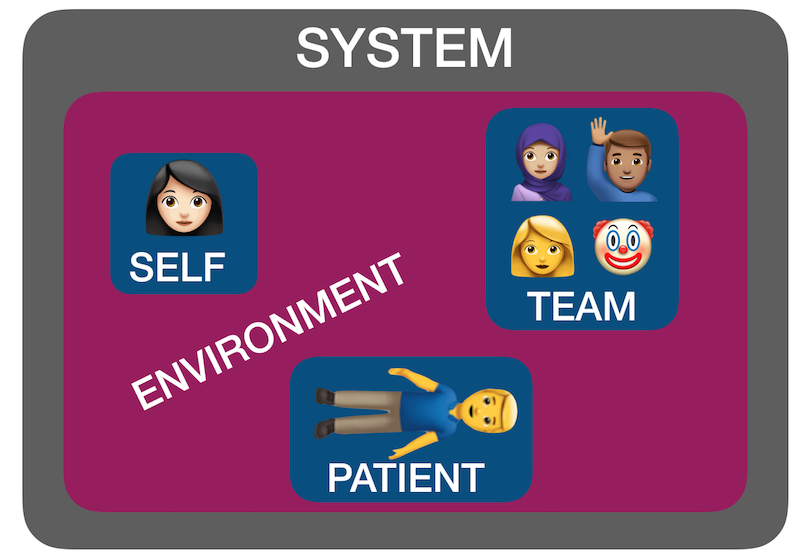
But ‘self, team, environment and patient’ isn’t just a useful system for case preparation. It can also be used for case analysis. I have found by discussing many ‘unsatisfactory’ cases over the years with participants in human factors workshops that STEP can help us identify where the issues lie. Accompanying all these factors is another ’S’: the system in which they interplay – the organisational rules, processes, policies, resources and deficiencies that may facilitate or obstruct an effective resuscitation(2).
Using STEPS to analyse cases The following (genuinely) hypothetical resus cases demonstrate how the application of this framework – Self, Team, Environment, Patient, System – might help identify correctible factors for future resuscitations:
1. Cardiac arrest in the bathroom on the orthopaedic ward – “it was chaos, there were too many people, and the resus trolley wasn’t properly stocked”.
STEPS analysis: Team – Leader needed to assign roles and allocate tasks Environment – Crowd control needed, lack of equipment System – Adequate checks for resus trolley not in place
2. 19-year-old male stabbed in the chest and arrested on arrival in hospital. CPR provided but went from PEA to asystole. Team leader discontinued resus after 20 minutes. Resident: “I thought he needed a resuscitative thoracotomy but no-one was willing to do it. No-one even mentioned it”.
STEPS analysis: Self – Lacked confidence to speak up, doubted own knowledge or influence Team – Lack of team situational awareness or knowledge or skill regarding required intervention System – Insufficient training and preparation for penetrating traumatic cardiac arrest scenario
3. 30-year-old mother with abdominal wound and her 2-year-old daughter with massive open head injury, both due to gunshot wounds, having been shot by husband/father who killed himself on scene. Child arrests in the ED, without ROSC, witnessed by mother before mother is taken to operating theatre.
STEPS analysis: Patient(s) – tragic case with upsetting circumstances and compounded psychological distress for patient and staff. The best resuscitation team in the world is not going to feel good about this one.
4. 46-year-old previously healthy male with VF arrest achieved ROSC after prehospital defibrillation and brought to the ED of a non-cardiac centre comatose and intubated. Further refractory VF in ED. Received multiple shocks, antiarrhythmics, double sequential external defibrillation. No on-site access to mechanical CPR, cardiac catheterisation, or ECMO. Patient declared dead in ED.
STEPS analysis: System – Prehospital team gave excellent care but brought the patient to a hospital ill-equipped to manage his ongoing needs, due to lack of ambulance service policy regarding appropriate destination hospital for cardiac arrest cases.
Summary You can see from the above cases how STEPS may be applied to make some sense of where a resus has gone wrong. Note that I am not recommending this as a way of structuring a team debrief or formal incident investigation – many institutions already have processes for conducting these and various rules and sensitivities have to be accommodated. Rather, this is a format I’ve found helpful in applying during informal discussions that aim to get the nub of where things could or should have gone better.
Occasionally, you can get a case where the STEPS seem to be aligned but things still feel bad – in which the outcome was unsatisfactory because the plan was wrong, or the team wasn’t able to execute the plan. In my next post I’ll discuss another way of analysing cases that can accompany STEPS.
They say emergency medicine and critical care are no picnic, but I’ve been trying to change that. There’s something about sitting down on a blanket and sharing protected time for conversation that makes for good team building and effective communication. If you have snacks, it’s even better.
In the emergency department or intensive care unit one sometimes has to be opportunistic regarding finding time for teaching, debriefing a resuscitation case, or even eating. We end up doing these things (if at all) on the fly, in a rushed manner, and often standing up. Do we really have to? All you need for a picnic is a blanket, a floor, and some people. Hospitals have these. If you don’t want to be seen, pop outside or use a bed space with a curtain round it.
Picnic Debrief
Here’s an example of an impromptu picnic. It was late in the evening, early 2013. After two busy resus cases, my senior registrar and I debrief picnic-style, with potato chips from a vending machine and a nice pot of tea. We’re still in the ED and available to our team, but anyone can clearly see we’re in the ‘picnic zone’ and so we’re left alone for ten minutes to gather our thoughts and identify any learning points. The ED is usually a factory of interruption, but no-one wants to interrupt a picnic.
Picnic Teaching
Here’s resident teaching. We don’t have time to leave the ED, but there’s always time for a picnic, during which we cover a surprising number of critical care topics. People won’t fall asleep while picnicking.
Picnic Picnic
And here’s a picnic with the intensive care trainees outside the unit. This is actually lunch, but why shouldn’t lunch be a picnic once in a while?
We’re encouraged to practice mindfulness and take mental time out as a way to prevent or manage stress in the critical care environment. I think this is enhanced with an accompanying brief physical time out too. One person sitting on a blanket on the floor might be a weirdo. Get two or more people, and you have a picnic. Everyone loves a picnic.
‘Do what you said you were going to do – the high performance culture of excellence under pressure’ is the title of a talk by General John Jansen, organised by my friend A/Prof Brian Burns on behalf of Sydney University.
It will be held on 20 December at 18.00 hrs at the Royal Prince Alfred Hospital in Sydney.
Free Registration available here, and refreshments are provided.
My whole career has been about finding ways to optimise resuscitation. Many others also have the bug. The ‘resuscitationist movement’ is sweeping across Europe, with Katrin Hruska and Femke Geijsel about to run amazing courses for emergency teams in Sweden and The Netherlands. I have the honour of joining Clare Richmond in helping them do that. But first Critical Care in the Emergency Department is going to be run in London one more time.
This course contains the stuff I wish someone had told me as a registrar. A synthesis of my learning points in intensive care, prehospital & retrieval medicine, paediatric critical care, and being a front line ED doc for 20 years.
I’ve been running the course for over a decade, including in London, Birmingham, Basingstoke, Dublin, Stockholm, Sydney and Maribor. Each time I try to improve it, and try to squeeze one or two more learning points in. It’s a tough day – just me and fifty or so critical care cases to talk about. But no-one goes to sleep – guaranteed! Everyone has to work – to talk, think, and interact.
It is of course primarily a clinical course, focusing on optimal clinical practice. But consistent feedback from participants is that they get far more from it: a reassurance that they’re not crazy wanting to do more for their patients, and a way forward for remaining inspired and motivated to make changes to their practice and to their departments.
I’ve always had strong feelings about education. I was an uninspired and underachieving medical student, exasperated at the fact that the preclinical course at my medical school consisted of lengthy lectures about detailed aspects of basic sciences like histology and embryology. To make it worse, the teaching was delivered by basic science PhD students who were required to teach medical students as part of their contract. They taught because they had to, not because they were good at it. In other words, the best way to summarise how I was initially taught to be a doctor is this: my medical training consisted of being taught stuff I didn’t need to know, by people who weren’t doctors, and who didn’t know how to teach.
This frustrated me enormously. It wasn’t until I hit the wards as a senior medical student and then junior doctor that I would occasionally run into enthusiastic and supportive clinicians who were keen to share what they knew. They seemed to be few and far between, but the crumbs they dropped were enough to leave a trail that led me to be determined to become a doctor who could similarly inspire and motivate others to love learning.
Throughout my training I made a consistent observation: a small amount of good education was extremely motivating. The converse was also true – being denied access to education was extremely demotivating. In one department, teaching was continually cancelled due to patient load. When questioned on this, the clinical director stated “teaching is a privilege, not a right”. This influenced me profoundly, because I immediately adopted that phrase as a personal motto, except that I flipped the order of “right” and “privilege”.
A few events have converged this week to remind me of the power of good education. The first, and most important, was when my friend Rob Rogers, a renowned emergency medicine educator who has run courses on how to teach all over the world, tweeted a picture of an interesting ECG.
Rob and his team have inspired so many people with their brilliant education. Faced with a life-threatening ST-elevation MI, Rob chose to share his ECG with his Twitter followers. Later he shared details of his angiogram pre- and post-revascularisation. Now THAT is commitment to education!
The second event this week is that we are running our Sydney HEMS induction course in prehospital & retrieval medicine. This is about as full on as medical education can get, with hours of simulation, testing, and stress exposure. I am constantly amazed at the dedication and hard work of my colleagues who make up the course faculty, and the willingness of the participants to go the extra mile to improve their performance. We have the honour of inviting medics from certain branches of the Australian military to attend the course, and one such armed forces ‘graduate’ of our course recently contacted me:
He attached a document outlining a situation he faced which took my breath away. I’m not yet allowed to share it, but the bravery he showed was awe-inspiring. To think that he credits some of his preparation to the training we gave is truly humbling. It is also a reminder of the enormous responsibility of educators.
We can provide both negative and positive inspiration through our choices in what we say and how we say them, and in the teaching we deliver. As learners those educational experiences shape us and stay with us forever, influencing the choices we make and how we choose to pass on the teaching.
The humbling feedback from my military friend along with Rob’s ongoing desire to educate in the face of life-threatening illness serve to remind us of the power of education, and the responsibility we educators have to share, to inspire, and to provide the highest quality teaching.
Something Rob already seems to be working on, less than a week post-myocardial infarction …
@hayleybsa 8am on the 14th…working on the schedule now…Course is going to be FANTASTIC!
I love education. As a trainee, I was lucky to be guided by a handful of excellent mentors along the path. The truth is however, in many places I worked inspiration and good education were hard to find.
I am driven by the desire to make my trainees and colleagues better than me. As a critical care physician, I can only save so many lives in one career. But as an educator I have an opportunity to influence patient care in regions of spacetime to which I will never have personal access.
A massive investment has gone into my medical education. My parents worked their butts off to allow me to study. State funded university education in England got me my medical degree. Taxpayers’ money paid my salary throughout my training. Most importantly, thousands of patients put their trust in me as I did my best to learn medicine by treating them, sometimes getting it right, often getting it less than optimal. I owe all of them. I owe it to them, and to myself, to make it all count as much as possible.
If I can ignite a spark in a trainee’s mind that inspires them to improve, or share a memorable clinical tip that gets recalled and applied at a critical point in a resuscitation months or years from now, then all that investment, all that sacrifice, is so much more worth it.
Here’s a list of the principles I try to apply, especially when running courses. Underlying all of this is the goal to provide the kind of training I would have loved to have received myself.
Cliff’s Clinical Teaching Tips
Keep it case-based
This allows the nurse, the specialist, and intern to be in the same classroom. When we’re considering patients, everyone can learn something that is relevant to their professional perspective and experience.
Respect the learner
Allow everyone to question the teaching and express their opinion. Never humiliate anyone. The less threatened people feel, the more exploratory their questions will be, and the better they are able to make sense of the information discussed.
Have regular breaks, with food, water, and caffeine
If people have travelled to learn, they need to be protected from fatigue, dehydration, neuroglycopaenia and caffeine withdrawal. If they know you care about these things, they know you care about an effective learning environment, and will be more engaged.
How to make it memorable
Make it fun
Learning is great fun. We should have a good time together. If you’re bored, you won’t learn effectively. Funny or unusual stuff is more memorable, too.
Connect emotionally
Critical care is emotive. During resuscitation we have powerful interactions with ourselves and with our colleagues, sometimes negatively. Learners who are experienced clinicians have all felt pain or frustration in the resuscitation environment. Addressing these issues, by focusing on what could be done better, from a self, team, environment, or systems point of view frames the clinical teaching in more realistic and more applicable context. Sharing my own feelings about cases I’ve managed shows the learners how similar we all are inside, and I’ll be better able to convince them that they are just as capable of applying what is taught as I am. We can advise learners more effectively how to think and behave if we immerse the teaching in the reality of human experience.
Keep it simple
A quotation often misattributed to Einstein is “If you can’t explain it simply, you don’t understand it well enough”. Resuscitation and critical care concepts, certainly as applied to the initial resus room evaluation and therapies, can all be explained in uncomplicated ways. It behooves any resuscitation educator to adhere to this.
Have a framework that you continually refer back to
Knowing where to ‘store’ new information and how it relates to existing knowledge or other concepts being taught is important for understanding and retention. A classic example of such a framework is the ABCDE primary survey, but many more can be created. It also facilitates communication of ideas though mindmaps or note taking via sketchnotes.
Tell stories
This relates to connecting emotionally, as recommended above, but there is more to it. Humans have communicated information and ideas through storytelling since the dawn of civilisation. We are hardwired so that our attention is captured by stories.
Use mnemonics
Mnemonic tools like acronyms are helpful for information that needs to be rapidly accessed, like the one I made for possible causes of a raised lactate when you’re looking at a blood gas from a patient in the resus room with a lactate of 12 mmol/l.
I’ve been in the privileged position of being able to apply these principles in courses I’ve run in various countries for over a decade. In 2016 I get to do it again in the Netherlands, Sweden, and England. I’m one very lucky educator!
This talk was the opening plenary given at smacc Chicago. The title they gave me was ‘Advice To A Young Resuscitationist. It’s Up To Us To Save The World‘ but I ditched the last half because, as I point out later in the talk, I don’t think it is up to us to save the whole World. Some AV muppetry at the conference centre prevented the smacc team from being able to include the slides, so I’ll post those too at some point. You can hear the talk as a podcast at the ICN or on iTunes
Last weekend I got my butt handed to me and I’m feeling really good about it. I entered my first Brazilian Jiu Jitsu competition, and was beaten unequivocally, having had to submit to avoid having my arm broken after about three minutes into the fight. So what’s to be so cheerful about? Essentially, the whole endeavour was an experiment, and the experiment was a success. I learned a heap about learning, and about myself. Lessons that can be applied to learning resuscitation medicine, or learning anything.
The 10000 hours fallacy: not all hours are created equal
I’ve been doing Brazilian Jiu Jitsu (BJJ) for about a year, and am not very good at it. I started it because my (then) five year old son started it, and I thought it would be nice if we could share an interest in something healthful and useful for self protection. For most of that year I made 1-2 sessions a week, usually rushing to class after an emergency department or retrieval medicine shift and not really having my ‘head in the game’. Turning up. Just like it’s possible to turn up to work, get through your shift, and go home and forget about it.
I noticed something interesting about the people who started around the same time as me. Those who were entering competitions – as inexperienced and ill-prepared as they were in the beginning – progressed much faster than me. They would break down techniques and work on specific movements or positions they knew they needed to improve because of their competition experience, and they’d ask targeted questions of the coaches, aimed at maximising feedback for them to work on. It dawned on me that I was witnessing something I’d described in a lecture on Cutting Edge Resuscitation performance at the Royal College of Emergency Medicine Conference last year:
“What seems to be apparent is that although many hours of practice are important, pure exposure or experience alone does not predict those who will master their subject. We may have all encountered colleagues who have many years under their belt who lack that spark you’d expect of a cutting edge expert. So merely turning up to work every day doesn’t make you better, it just makes you older. You reach a certain level where you can manage the majority of cases comfortably, after which more exposure to the same experience fails to improve performance expertise.
What differentiates the cutting edge performers from the majority in all these domains (studied areas such as chess or sports or music) appears to be the amount of deliberate practice, or effortful practice, in which individuals engage in tasks with the explicit goal of improving a particular aspect of performance, and continue to practice and modify their performance based on feedback, which can come from a coach or mentor or the results of the performance itself.”
“Competence does not equal excellence” – Weingart
With this realisation, I decided to enter a competition I was extremely unlikely to win. I knew that committing (publicly) to a deadline would force me to improve my game, and I turned up more, studied the notes I’d made, and started asking more questions. In the space of a few weeks I felt that my BJJ was progressing faster than before.
The powerful combined forces of deadlines and public commitment
There’s nothing like a deadline or a high stakes test or exam to focus the mind. I’ve done several postgraduate fellowships and diplomas by examination, some of which were optional, and I’m sure each one raised my knowledge and clinical ‘game’ more than any other educational intervention I can think of.
The reality of the competition day approaching forced me to tackle my training, fitness, diet and timetable in a way I otherwise would not have found the motivation for. I had a strange moment when I took off my teeshirt in the changing rooms prior to the match and caught sight of my reflection in the mirror. I barely recognised how different my physique was compared with months earlier. Previously, I’d exercised for its own sake and not made much progress losing the middle aged paunch. But the public commitment to a BJJ fight, in a certain weight category, instilled the drive to exercise and monitor my diet. Commitment to this deadline physically restructured me!
Stress exposure training WORKS!
I’ll be 49 this year. The only people available in my weight category to fight me were aged 36-40. Age can make a big difference. Injuries are not uncommon and a significant one could put me out of training or out of work. My wife and son and friends were going to watch me, and I didn’t want to let them down or put on a pathetic performance. All my buddies who had competed before warned me of the overwhelming nervousness that can disorientate you and cloud your concentration. There were plenty of potential negative outcomes to focus on, but I ignored them all. I knew the simple formula. Breathe. Talk. See.
This basic mantra, assisted by the mnemonic ‘Beat The Stress’ (BTS) developed by Michael Lauria, is something we teach and apply in the training department of Sydney HEMS. Breathe means control and pay attention to your breathing, allowing you to reduce sympathetic hyperactivation and be ‘in the moment’. Talk means positive self-talk: a silent internal monologue that reminds yourself of all the preparation you’ve done and the potential positive outcomes of the task about to be performed. See means visualise: run through in your mind a successful performance, imagining yourself overcoming any anticipated obstacles – a practice which prepares your mind and body for effective task execution.
Less than a week ago I was running workshops on human factors for Sydney University Masters of Medicine (Critical Care) students, and covered how we submit our new HEMS clinicians to stress exposure training in order for them to practice Lauria’s BTS approach. Throughout these workshops I couldn’t wait for the opportunity to test what I teach.
On the day, my only interpretation of my adrenal surge was excitement. Even in the ‘holding pen’ after weigh-in where you wait with other competitors to have your bout, there was no anxiety, no fear. I couldn’t wait to get on the mat. The whole thing was an exhilarating buzz, and even when the can of whoopass was being unloaded on me I felt cognitively ‘available’: aware of my surroundings (and predicament!) and able to control my breathing while I self-talked my way through my limited and ever dwindling options.
Conclusion
It might be slightly unusual to be singing from the rooftops about a defeat, but the educational principles I’m re-learning are worth re-sharing. I took myself out of a comfort zone, and made a public commitment to be tested. This focused my learning and made me practice in a different way and more proactively seek feedback. I no longer was ‘turning up’, I was training towards a goal. This renewed sense of ownership of my training transformed my level of engagement in the learning process, instilling an enthusiasm and craving to understand and test principles rather than rote learn techniques. I had an opportunity to test ‘Beat The Stress’ in a non-clinical setting and this mindware tool proved itself yet again. And despit
e the uninspiring outcome on the day, I was back sparring the following evening, with an even greater hunger for specific answers from the coaches, and with senior students remarking ‘you’ve got better’.









 ‘Do what you said you were going to do – the high performance culture of excellence under pressure’ is the title of a talk by General John Jansen, organised by my friend
‘Do what you said you were going to do – the high performance culture of excellence under pressure’ is the title of a talk by General John Jansen, organised by my friend 

 I’ve always had strong feelings about education. I was an uninspired and underachieving medical student, exasperated at the fact that the preclinical course at my medical school consisted of lengthy lectures about detailed aspects of basic sciences like histology and embryology. To make it worse, the teaching was delivered by basic science PhD students who were required to teach medical students as part of their contract. They taught because they had to, not because they were good at it. In other words, the best way to summarise how I was initially taught to be a doctor is this: my medical training consisted of being taught stuff I didn’t need to know, by people who weren’t doctors, and who didn’t know how to teach.
I’ve always had strong feelings about education. I was an uninspired and underachieving medical student, exasperated at the fact that the preclinical course at my medical school consisted of lengthy lectures about detailed aspects of basic sciences like histology and embryology. To make it worse, the teaching was delivered by basic science PhD students who were required to teach medical students as part of their contract. They taught because they had to, not because they were good at it. In other words, the best way to summarise how I was initially taught to be a doctor is this: my medical training consisted of being taught stuff I didn’t need to know, by people who weren’t doctors, and who didn’t know how to teach.



