This video shows the mechanism for dislodgement and deformation of humeral intraosseous needles and how to avoid this.
In summary, if you need to abduct the arm (eg. for thoracostomy), keep the thumbs down (ie. have the arm internally rotated at the shoulder). Otherwise the IO catheter may bend or fall out.
Occasionally we step out of the resuscitation room feeling like a case should have gone better, but it can be hard to put our finger on just where it went wrong. In my last post I discussed the STEPS approach to analysing resuscitation cases: Self, Team, Environment, Patient and System.
Occasionally you can get a case where the STEPS seem to be aligned but things still feel bad. In which the outcome was unsatisfactory because the plan was wrong, or the team wasn’t able to execute the plan. Consider the following case.
1. A patient with a past history of DVT no longer on anticoagulants presents with chest pain and syncope.
She is severely hypotensive with a raised jugular venous pressure and a clear chest x-ray. A working diagnosis of pulmomary embolism is made.
Discussions ensue regarding empirical fibrinolysis and a respiratory physician is consulted, who over the phone cautions against treating without a CT pulmonary angiogram.
The patient is given heparin and transferred to the CT scanner where she arrests. Intravenous rtPA is given during CPR but no return of spontaneous circulation is achieved and she is pronounced dead after 30 minutes of resuscitation.
On this occasion the team worked efficiently and communicated well under clear leadership. Everyone knew the plan and shared the mental model. The environment was well controlled and the patient had been swiftly moved to CT within 20 minutes of arrival. Thanks to simulation training the well rehearsed cardiac arrest resuscitation was conducted with precision and the team was able to rapidly access the thrombolytic and knew the correct dose.
By a quick STEPS analysis, this case appears to have gone as well as could be expected. Perhaps there is nothing to learn. Some you win, some you lose, no?
No. Autopsy revealed type A aortic dissection with pericardial tamponade.
The management may have been efficient but it failed to be effective. In other words, things were done right, but the right things weren’t done; they did the wrong things right.
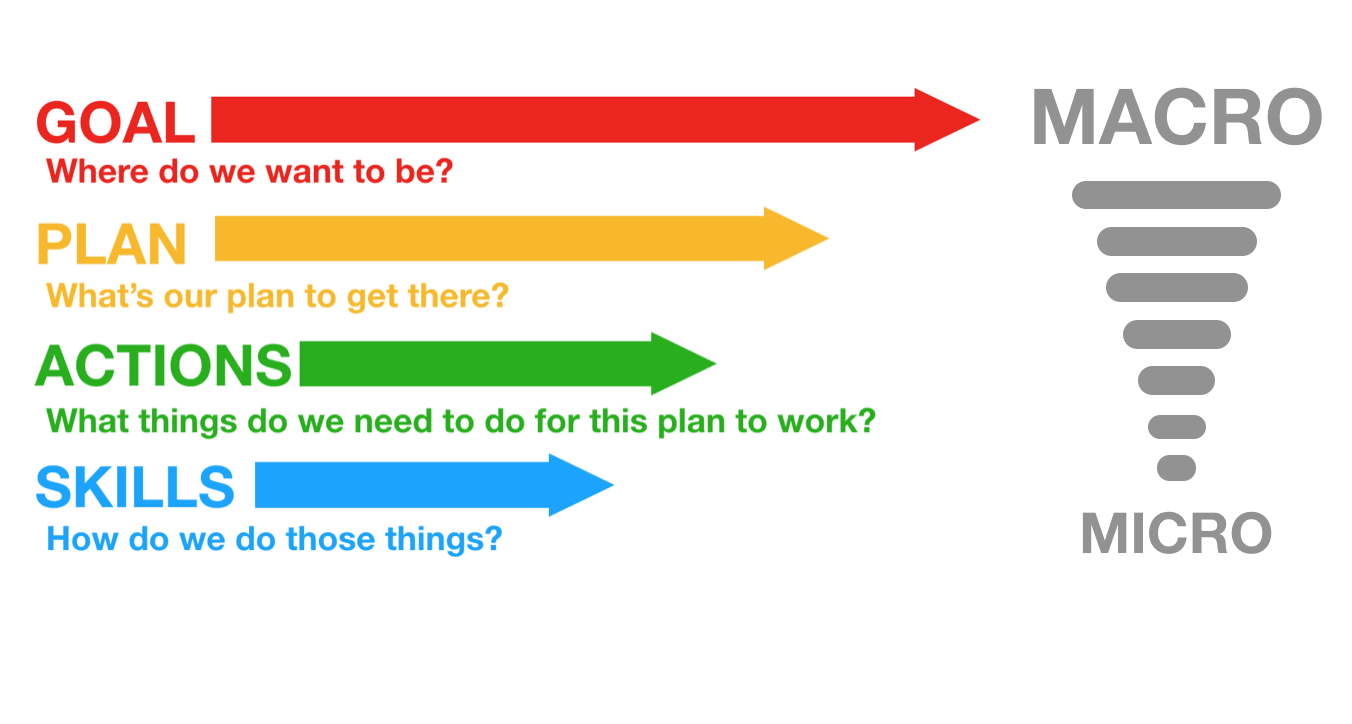
This might be an example where STEPS is inadequate, and instead we should evaluate the clinical trajectory. The cognitive bias that led to a lack of consideration of alternative diagnoses might be classifiable under ‘self’ or ‘team’ but I find it more helpful to consider it under a failure of strategy. What is strategy? Strategy in my mind is another word for plan. The plan is based on a particular resuscitation goal, and will consist of the procedures & skills required to action the plan. We can thus break down an attempted clinical trajectory into:
Goal (what are we trying to achieve) Strategy, or Plan (what’s our plan to get there?) Tactics, or Actions (what procedures will be required to execute the plan) And, at more granular level: If we’re failing at the procedural level, the components of procedures, namely Skills & Microskills. So, as we zoom in from macro to micro in setting the clinical trajectory, we can look at Goals, Plan, Actions, and Skills: In the above case it appears the following was applied, in terms of Goal-Plan-Actions-Skills:
G – resuscitate hypotensive patient P – give fibrinolysis for likely PE A – consult respiratory physician, get CTPA S – request scan, give heparin, transport to CT
The goal was appropriate, but the plan was ineffective.
The following approach would have been more effective.
G – resuscitate hypotensive patient P – identify cause of undifferentiated hypotension and initiate treatment in the resus room A – thorough bedside assessment in patient too sick to move: history, physical, CXR, ECG, labs, POCUS S – Basic cardiac ultrasound
By planning to identify and treat the cause of hypotension in the resus room, the more appropriate investigation would have been selected (cardiac ultrasound) and the correct diagnosis is much more likely to have been made.
Let’s look at some other cases:
2. An 88-year-old male presents by ambulance to the ED with dizziness. He is hypotensive, pyrexial, hypoxic and confused.
His chest x-ray shows likely bronchopneumonia. He has appropriate initial resuscitation and ICU is consulted. Soon he is intubated and on high dose vasoactive medication with escalating doses despite ongoing hypotension, anuria, and a lactate of 11 mmol/l, increased from 8 on arrival.
As he is being wheeled off down the corridor towards ICU his distraught and frail wife arrives. She is taken to the quiet room where she explains that her husband would never want to be ‘on a life support machine’ and asks ‘can’t you just keep him comfortable’?
G – the goal – to provide maximally aggressive resuscitation – was not in keeping with the patient’s wishes. If the goal had been to provide care in accordance with his wishes, the plan could have included attempts to ascertain these sooner while providing initial treatment. Upon gaining sufficient information, a new goal can be established: maximising the patient’s comfort and dignity.
3. An obese 30-year-old female presents with syncope. At triage she is pale, tachycardic & hypotensive. Clinical and sonographic assessment, including free intraperitoneal fluid and a positive urine HCG, is suggestive of ruptured ectopic pregnancy.
The gynaecologist and anaesthetist ask the ED team to bring the patient straight to the operating room. The ED team spends 20 minutes struggling to obtain intravenous access, eventually placing a 22G intravenous catheter in the patient’s hand and a humeral intraosseous needle.
Her shock is considerably worse on arrival in theatre, despite attempts to transfuse O negative blood en route.
Goal – get her safely to the operating room Plan – vascular access, cross match blood, start haemostatic resuscitation, go to OR as soon as possible Actions – peripheral and/or intraosseous cannulation attempts Skills – vascular access skills
Here the failure was at the actions and skills level. Better vascular access could have been attained using ultrasound guided peripheral cannulation, or central vascular access, or earlier intraosseous insertion.
4. A 120kg 32-year-old male with a history of deliberate self harm presents on the night shift with coma due to mixed benzodiazepine and venlafaxine overdose.
The decision is made to intubate for airway protection. After rapid sequence induction direct laryngoscopy is attempted by the emergency registrar who obtains a grade 4 view. Cricoid pressure is removed resulting in a grade 3 view.
The registrar asks for a bougie which she passes and then railroads the tracheal tube over it. The cuff is inflated, capnography is connected, and the self-inflating bag is connected and squeezed while the chest is auscultated.
The abdomen distends, the capnograph remains flat, and gastric contents are seen to pass upward through the tube into the self-inflating bag. The tube is immediately removed and bag-mask ventilation is attempted. The oxygen saturation is now 78% and the airway is soiled. The airway is suctioned and repeat attempts to bag-mask ventilate fail. A successful cricothyroidotomy is performed and the patient subsequent has full neurological recovery.
Goal – Provide supportive care and minimise complications from overdose Plan – Airway protection and admit to ICU for monitoring Actions – Rapid sequence intubation, ICU referral Skills – Pre-, peri- and post-intubation oxygenation techniques; patient positioning; rapid sequence induction of anaesthesia; direct laryngoscopy; bougie handling techniques; external laryngeal manipulation
In this case the patient was not placed in the ramped position and no nasal cannulae were applied for apnoeic oxygenation. A tube was railroaded over an oesophageal bougie, which arguably should not occur if ‘hold up’ is sought when the bougie is placed.
Although the goal, plan and actions were appropriate, the team did not demonstrate adequate skill in this procedure. Likely due to a failure of training, standardised procedures, and checklists (or their application), this could also be identified as a ‘system’ problem in STEPS. It is also possible that the intubator forgot her training under stress – a problem classifiable under ‘self’. Alternatively other members of the team may have had knowledge but didn’t speak up or cross-check their colleague, which would be a ‘team’ issue.
Limitations of this approach This sort of analysis is retrospective and subjective and at risk of hindsight bias (e.g. distortion due to projection, denial, or selective recall). However, these limitations do not negate the value of the learning exercise, particularly if we are aware of them and strive to minimise their impact (e.g. write down the details of a cases as soon as possible afterward). It at least provides a structure for individuals and teams to begin the conversation about where and how things may have been suboptimal.
Goals may be multiple and may change according to incoming information, and for each goal there may be several viable alternative plans. STEPS and GPAS may overlap, eg. team failures may result in inappropriate goals and strategies, or in failed procedures.
Summary These models may prove helpful as a means of dissecting a case in a structured way. Put simply, STEPS offers a structure for identifying efficiency improvements (“doing things right”) and GPAS can help us assess effectiveness (“doing the right things”).
Another way of looking at it is that STEPS provides the components of a resus at any point in time, and GPAS defines the trajectory: where the resus is going and how to get there.
I use this structure to analyse cases in my own clinical practice and in my teaching. I would be interested to hear from others’ experience. Do you find this approach useful in identifying areas for improvement in those cases that you feel should have gone better?
Thanks to Chris Nickson for his comments and improvements to this post
A resuscitationist agonises. These words, expressed by Scott Weingart during a podcast we did together, ring true to all of us who strive to improve our practice. Driven by the passionate conviction that we should never lose a salvageable patient through imperfect care, we relive cases and re-run them through our mental simulators to identify areas for improvement.
In the search for actionable items though, we occasionally exit this process empty-handed. Something about a case felt wrong although ostensibly all the clinical interventions may have been appropriate. It is in these cases that it can be helpful to have a structure to aid analysis.
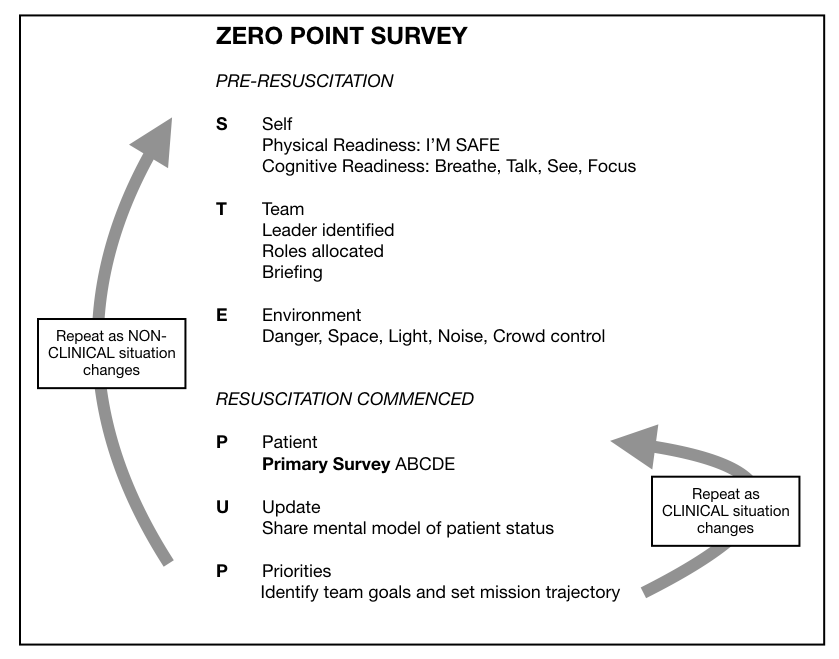
I, along with an international, interdisciplinary faculty of resuscitationists, have previously proposed an easily remembered system for optimising the clinical and non-technical components of resuscitation immediately before and during a patient encounter, dubbed the ‘Zero Point Survey’ (ZPS)(1), so called because first contact with a patient is rarely ‘Time Zero’ for a prehospital mission or hospital resuscitation case; there is invariably time for preparation of oneself, one’s team, and the environment (including equipment) prior to the primary survey and commencement of resuscitation. Following the assessment and management of STEP (self, team, environment & patient), the team should be regularly Updated on patient status and informed of the Priorities.
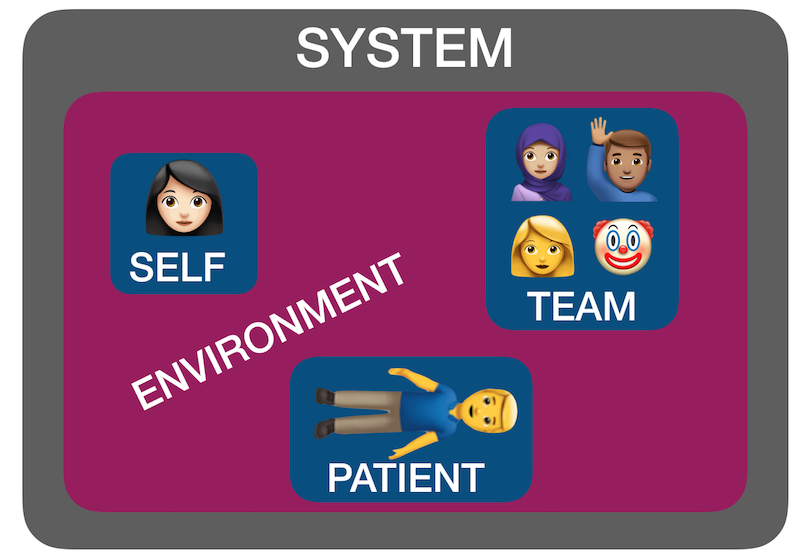
But ‘self, team, environment and patient’ isn’t just a useful system for case preparation. It can also be used for case analysis. I have found by discussing many ‘unsatisfactory’ cases over the years with participants in human factors workshops that STEP can help us identify where the issues lie. Accompanying all these factors is another ’S’: the system in which they interplay – the organisational rules, processes, policies, resources and deficiencies that may facilitate or obstruct an effective resuscitation(2).
Using STEPS to analyse cases The following (genuinely) hypothetical resus cases demonstrate how the application of this framework – Self, Team, Environment, Patient, System – might help identify correctible factors for future resuscitations:
1. Cardiac arrest in the bathroom on the orthopaedic ward – “it was chaos, there were too many people, and the resus trolley wasn’t properly stocked”.
STEPS analysis: Team – Leader needed to assign roles and allocate tasks Environment – Crowd control needed, lack of equipment System – Adequate checks for resus trolley not in place
2. 19-year-old male stabbed in the chest and arrested on arrival in hospital. CPR provided but went from PEA to asystole. Team leader discontinued resus after 20 minutes. Resident: “I thought he needed a resuscitative thoracotomy but no-one was willing to do it. No-one even mentioned it”.
STEPS analysis: Self – Lacked confidence to speak up, doubted own knowledge or influence Team – Lack of team situational awareness or knowledge or skill regarding required intervention System – Insufficient training and preparation for penetrating traumatic cardiac arrest scenario
3. 30-year-old mother with abdominal wound and her 2-year-old daughter with massive open head injury, both due to gunshot wounds, having been shot by husband/father who killed himself on scene. Child arrests in the ED, without ROSC, witnessed by mother before mother is taken to operating theatre.
STEPS analysis: Patient(s) – tragic case with upsetting circumstances and compounded psychological distress for patient and staff. The best resuscitation team in the world is not going to feel good about this one.
4. 46-year-old previously healthy male with VF arrest achieved ROSC after prehospital defibrillation and brought to the ED of a non-cardiac centre comatose and intubated. Further refractory VF in ED. Received multiple shocks, antiarrhythmics, double sequential external defibrillation. No on-site access to mechanical CPR, cardiac catheterisation, or ECMO. Patient declared dead in ED.
STEPS analysis: System – Prehospital team gave excellent care but brought the patient to a hospital ill-equipped to manage his ongoing needs, due to lack of ambulance service policy regarding appropriate destination hospital for cardiac arrest cases.
Summary You can see from the above cases how STEPS may be applied to make some sense of where a resus has gone wrong. Note that I am not recommending this as a way of structuring a team debrief or formal incident investigation – many institutions already have processes for conducting these and various rules and sensitivities have to be accommodated. Rather, this is a format I’ve found helpful in applying during informal discussions that aim to get the nub of where things could or should have gone better.
Occasionally, you can get a case where the STEPS seem to be aligned but things still feel bad – in which the outcome was unsatisfactory because the plan was wrong, or the team wasn’t able to execute the plan. In my next post I’ll discuss another way of analysing cases that can accompany STEPS.
I find clinicians are quick to consider sepsis and hypoperfusion/ischaemia as causes of a raised lactate, but slow to include other causes in their differential.
Although an elevated lactate has been shown to be associated with worse outcomes in numerous studies, not all causes of a raised lactate are sinister. It’s therefore important to diagnose the cause both to allow the right treatment and to avoid assuming an inappropriately poor prognosis.
This 12 minute video offers an approach to diagnosing the cause of elevated lactate based on an understanding of lactate physiology using a simple visual aid – a ‘lactate map’ and a memorable acronym.
Reference
1. Reid C, Rees V, Collyer-Merritt H. Non-septic hyperlactataemia in the emergency department. Emerg Med J. 2010 May;27(5):411–2
Mention the term ‘difficult airway’ and many of us will conjure mental images of some kind of distorted anatomy. However, airway management may be ‘difficult’ for a number of reasons, and no internationally agreed definition of the term exists. Given the wrong staff and circumstances, an ‘easy’ airway in your or my hands may indeed become very difficult. In their editorial “The myth of the difficult airway: airway management revisited” (1) Huitink & Bouwman state:
“In our opinion, the ‘difficult airway’ does not exist. It is a complex situational interplay of patient, practitioner, equipment, expertise and circumstances.”
Airways that are anatomically difficult (eg. limited mouth opening, short thyromental distance, large tongue, neck immobility, etc.) and physiologically difficult (hypoxaemia, hypotension, acidosis) are well described among FOAM resources (2-4). In addition to these, a third category of difficulty is well worth considering.
This last category probably surfaces more commonly than realised, particularly outside the operating room.
Imagine attending a cardiac arrest call on a medical ward. The patient is a 70 year old 120 kg male. The nurses have flattened the bed and discarded the pillow to optimise supine position for CPR. Gobs of vomitus splash from the patient’s pharynx with each compression. The wall suction system is disconnected. There is no bougie in the crash cart’s airway drawer. The nearest capnograph is on another floor of the hospital. In this scenario, no matter how excellent the critical care practitioner’s airway skills, this is a damned difficult airway.
I think Brindley’s third category is a term that should catch on, as a way of helping analyse cases that progress suboptimally and to identify factors during pre-intubation checks that can be addressed. It is terminology that I have added to my own Resuscitese Lexicon, particularly for case discussions during morbidity & mortality and airway audit meetings.
I would like to hear the ‘Situationally Difficult Airway‘ become more widely used, as it fills a gap in how we describe this important area of resuscitation practice.
This talk was the opening plenary given at smacc Chicago. The title they gave me was ‘Advice To A Young Resuscitationist. It’s Up To Us To Save The World‘ but I ditched the last half because, as I point out later in the talk, I don’t think it is up to us to save the whole World. Some AV muppetry at the conference centre prevented the smacc team from being able to include the slides, so I’ll post those too at some point. You can hear the talk as a podcast at the ICN or on iTunes
The use of inhaled nitric oxide is established in certain groups of patients: it improves oxygenation (but not survival) in patients with acute respiratory distress syndrome(1), and it is used in neonatology for management of persistent pulmonary hypertension of the newborn(2). But it can be applied in other resuscitation settings: in arrested or peri-arrest patients with pulmonary hypertension.
Read this (modified) description of a case managed by one of my resuscitationist friends from an overseas location:
A young lady suffered a placental abruption requiring emergency hysterectomy. She arrested twice in the operating room after suspected amniotic fluid embolism. She had fixed dilated pupils.
She developed extreme pulmonary hypertension with suprasystemic pulmonary artery pressures, and she went down the pulmonary HT spiral as I stood there. On ultrasound her distended RV was making her LV totally collapse. She arrested. Futile CPR was started.
I have never had an extreme pulmonary HT survive an arrest. I grabbed a bag and rapidly set up a manual inhaled Nitric Oxide system and bagged and begged…
She achieved ROSC after some minutes. A repeat ultrasound showed a well functioning LV and less dilated RV.
Today, after 12 hours she is opening her eyes and obeying commands. Still a long way to go, but alive.
It sounds impressive. I don’t have more case details, and don’t know how confident they could be about the diagnosis of amniotic fluid embolism but the presentation certainly fits with acute pulmonary hypertension with RV failure. The use of inhaled nitric oxide has certainly been described for similar scenarios before(3). But it raises bigger questions: is this something we should all be capable of? Are there cardiac arrests involving or caused by pulmonary hypertension that will not respond to resuscitation without nitric oxide?
Nitric oxide
Inhaled nitric oxide is a pulmonary vasodilator. It decreases right-ventricular afterload and improves cardiac index by selectively decreasing pulmonary vascular resistance without causing systemic hypotension(4).
RV failure and pulmonary hypertension
Patients may become shocked or suffer cardiac arrest due to acute right ventricular dysfunction. This may be due to a primary cardiac cause such as right ventricular infarction (always consider this in a hypotensive patient with inferior STEMI, and confirm with a right ventricular ECG and/or echo). Alternatively it could be due to a pulmonary or systemic cause resulting in severe pulmonary hypertension, causing secondary right ventricular dysfunction. The commonest causes of acute pulmonary hypertension are massive PE, sepsis, and ARDS(5).
The haemodynamic consequences of RV failure are reduced pulmonary blood flow and inadequate left ventricular filling, leading to decreased cardiac output, shock, and arrest. In severe acute pulmonary hypertension the RV distends, resulting in a shift of the interventricular septum which compresses the LV and further inhibits LV filling (the concept of ventricular interdependence).
What’s wrong with standard ACLS?
In some patients with PHT who arrest, CPR may be ineffective due to a failure to achieve adequate pulmonary blood flow and ventricular filling. In one study of patients with known chronic PHT who arrested in the ICU, survival rates even for ventricular fibrillation were extremely poor and when measured end tidal carbon dioxide levels were very low. In the same study it was noted that some of the survivors had received an intravenous bolus administration of iloprost, a prostacyclin analogue (and pulmonary vasodilator) during CPR(6).
CPR may therefore be ineffective. Intubation and positive pressure ventilation may also be associated with haemodynamic deterioration in PHT patients(7), and intravenous epinephrine (adrenaline) has variable effects on the pulmonary circulation which could be deleterious(8).
If inhaled nitric oxide (iNO) can improve pulmonary blood flow and reduce right ventricular afterload, it could theoretically be of value in cases of shock or arrest with RV failure, especially in cases of pulmonary hypertension; these are patients who otherwise have poor outcomes and may not benefit from CPR.
Is the use of iNO described in shock or arrest?
Numerous case reports and series demonstrate recovery from shock or arrest following nitric oxide use in various situations of decompensated right ventricular failure from pulmonary hypertension secondary to pulmonary fibrotic disease(9), pneumonectomy surgery(10), and pulmonary embolism(11) including post-embolectomy(12).
A recent systematic review of inhaled nitric oxide in acute pulmonary embolism documented improvements in oxygenation and hemodynamic variables, “often within minutes of administration of iNO”. The authors state that these case reports underscore the need for randomised controlled trials to establish the safety and efficacy of iNO in the treatment of massive acute PE(14).
Why aren’t they telling us to use it?
If iNO may be helpful in certain cardiac arrest patients, why isn’t ILCOR recommending it? Actually it is mentioned – in the context of paediatric life support. The European Resuscitation Council states:
ERC Guideline: (Paediatric) Pulmonary hypertension
There is an increased risk of cardiac arrest in children with pulmonary hypertension.
Follow routine resuscitation protocols in these patients with emphasis on high FiO2 and alkalosis/hyperventilation because this may be as effective as inhaled nitric oxide in reducing pulmonary vascular resistance.
Resuscitation is most likely to be successful in patients with a reversible cause who are treated with intravenous epoprostenol or inhaled nitric oxide.
If routine medications that reduce pulmonary artery pressure have been stopped, they should be restarted and the use of aerosolised epoprostenol or inhaled nitric oxide considered.
Right ventricular support devices may improve survival
Should we use it?
So if acute (or acute on chronic) pulmonary hypertension can be suspected or demonstrated based on history, examination, and echo findings, and the patient is in extremis, it might be anticipated that standard ACLS approaches are likely to be futile (as they often are if the underlying cause is not addressed). One might consider attempts to induce pulmonary vasodilation to improve pulmonary blood flow and LV filling, improving oxygenation, and reducing RV afterload as means of reversing acute cor pulmonale.
Are there other pulmonary vasodilators we can use?
iNO is not the only means of inducing pulmonary vasodilation. Oxygen, hypocarbia (through hyperventilation)(15), and alkalosis are all known pulmonary vasodilators, the latter providing an argument for intravenous bicarbonate therapy from some quarters(16). Prostacyclin is a cheaper alternative to iNO(17) and can be given by inhalation or intravenously, although is more likely to cause systemic hypotension than iNO. Some inotropic agents such as milrinone and levosimendan can lower pulmonary vascular resistance(18).
What’s the take home message?
The take home message for me is that acute pulmonary hypertension provides yet another example of a condition that requires the resuscitationist to think beyond basic ACLS algorithms and aggressively pursue and manage the underlying cause(s) of shock or arrest. Inhaled pulmonary vasodilators may or may not be available but, as always, whatever resources and drugs are used, they need to be planned for well in advance. What’s your plan?
Many clinicians extrapolate adult research findings to paediatric patients because there’s no alternative, and until now we’ve had to do that with post-cardiac arrest therapeutic hypothermia after paediatric cardiac arrest.
However the THAPCA trial in the New England Journal of Medicine now provides child-specific data.
It was a multicentre trial in the US which included children between 2 days and 18 years of age, who had had an out-of-hospital cardiac arrest and remained comatose after return of circulation. They were randomised to therapeutic hypothermia (target temperature, 33.0°C) or therapeutic normothermia (target temperature, 36.8°C) within 6 hours after the return of circulation.
Therapeutic hypothermia, as compared with therapeutic normothermia, did not confer a significant benefit with respect to survival with good functional outcome at 1 year, and survival at 12 months did not differ significantly between the treatment groups.
These findings are similar to the adult TTM trial, although there are some interesting differences. In the paediatric study, the duration of temperature control was longer (120 hrs vs 36 hrs in the adult study), respiratory conditions were the predominant cause of paediatric cardiac arrest (72%), and there were only 8% shockable rhythms in the paediatric patients, compared with 80% in the adult study.
The full text is available here. Therapeutic Hypothermia after Out-of-Hospital Cardiac Arrest in Children N Engl J Med. 2015 Apr 25
[EXPAND Abstract]
Background: Therapeutic hypothermia is recommended for comatose adults after witnessed out-of-hospital cardiac arrest, but data about this intervention in children are limited.
Methods: We conducted this trial of two targeted temperature interventions at 38 children’s hospitals involving children who remained unconscious after out-of-hospital cardiac arrest. Within 6 hours after the return of circulation, comatose patients who were older than 2 days and younger than 18 years of age were randomly assigned to therapeutic hypothermia (target temperature, 33.0°C) or therapeutic normothermia (target temperature, 36.8°C). The primary efficacy outcome, survival at 12 months after cardiac arrest with a Vineland Adaptive Behavior Scales, second edition (VABS-II), score of 70 or higher (on a scale from 20 to 160, with higher scores indicating better function), was evaluated among patients with a VABS-II score of at least 70 before cardiac arrest.
Results: A total of 295 patients underwent randomization. Among the 260 patients with data that could be evaluated and who had a VABS-II score of at least 70 before cardiac arrest, there was no significant difference in the primary outcome between the hypothermia group and the normothermia group (20% vs. 12%; relative likelihood, 1.54; 95% confidence interval [CI], 0.86 to 2.76; P=0.14). Among all the patients with data that could be evaluated, the change in the VABS-II score from baseline to 12 months was not significantly different (P=0.13) and 1-year survival was similar (38% in the hypothermia group vs. 29% in the normothermia group; relative likelihood, 1.29; 95% CI, 0.93 to 1.79; P=0.13). The groups had similar incidences of infection and serious arrhythmias, as well as similar use of blood products and 28-day mortality.
Conclusions: In comatose children who survived out-of-hospital cardiac arrest, therapeutic hypothermia, as compared with therapeutic normothermia, did not confer a significant benefit in survival with a good functional outcome at 1 year.
Some pectus excavatum patients have a metal ‘Nuss bar’ inserted below the sternum which can make chest compressions more difficult. In those without one, standard compression depths compress the left ventricle more than in non-pectus subjects, and might lead to myocardial injury.
This has led to a recommendation in the journal Resuscitation:
“Until further studies are available, we recommend strong chest compressions, according to the current guidelines, in PE patients with a sternal Nuss bar and, to minimize the risk of myocardial injury, we suggest a reduced chest compression depth (approximately 3–4 cm) at the level of lower half of the sternum in PE patients who have not had corrective surgery.”
Almost two-thirds of patients with extradural haematoma and bilateral fixed dilated pupils survived after surgery, with over half having a good outcome
Neurosurgeon, HEMS doctor, and all round good egg Mark Wilson was on the RAGE podcast recently and mentioned favourable outcomes from neurosurgery in patients with extradural (=epidural) haematomas who present with bilateral fixed dilated pupils (BFDP). Here’s his paper that gives the figures – a systematic review and meta-analysis.
A total of 82 patients with BFDP who underwent surgical evacuation of either subdural or extradural haematoma were identified from five studies – 57 with subdural (SDH) and 25 with extradural haematomas (EDH).
In patients with EDH and BFDP mortality was 29.7% (95% CI 14.7% to 47.2%) and 54.3% had a favourable outcome (95% CI 36.3% to 71.8%).
Only 6.6% of patients with SDH and BFDP had a good functional outcome.
Clearly there is potential for selection bias and publication bias, but these data certainly suggest an aggressive surgical approach is appropriate in some patients with BFDP.
The authors comment on the pessimism that accompanies these cases, which potentially denies patients opportunities for recovery:
“We believe that 54% of patients with extradural haematoma with BFDPs having a good outcome is an underappreciated prognosis, and the perceived poor prognosis of BFDPs (from all causes) has influenced decision making deeming surgery inappropriately futile in some cases.”
Scotter J, Hendrickson S, Marcus HJ, Wilson MH. Prognosis of patients with bilateral fixed dilated pupils secondary to traumatic extradural or subdural haematoma who undergo surgery: a systematic review and meta-analysis. Emerg Med J 2014 e-pub ahead of print Nov 11;:1–7
[EXPAND Abstract]
Primary objective To review the prognosis of patients with bilateral fixed and dilated pupils secondary to traumatic extradural (epidural) or subdural haematoma who undergo surgery.
Methods A systematic review and meta-analysis was performed using random effects models. The Cochrane Central Register of Controlled Trials and PubMed databases were searched to identify relevant publications. Eligible studies were publications that featured patients with bilateral fixed and dilated pupils who underwent surgical evacuation of traumatic extra-axial haematoma, and reported on the rate of favourable outcome (Glasgow Outcome Score 4 or 5).
Results Five cohort studies met the inclusion criteria, collectively reporting the outcome of 82 patients. In patients with extradural haematoma, the mortality rate was 29.7% (95% CI 14.7% to 47.2%) with a favourable outcome seen in 54.3% (95% CI 36.3% to 71.8%). In patients with acute subdural haematoma, the mortality rate was 66.4% (95% CI 50.5% to 81.9%) with a favourable outcome seen in 6.6% (95% CI 1.8% to 14.1%).
Conclusions and implications of key findings Despite the poor overall prognosis of patients with closed head injury and bilateral fixed and dilated pupils, our findings suggest that a good recovery is possible if an aggressive surgical approach is taken in selected cases, particularly those with extradural haematoma.






 The use of inhaled nitric oxide is established in certain groups of patients: it improves oxygenation (but not survival) in patients with acute respiratory distress syndrome(1), and it is used in neonatology for management of persistent pulmonary hypertension of the newborn(2). But it can be applied in other resuscitation settings: in arrested or peri-arrest patients with pulmonary hypertension.
The use of inhaled nitric oxide is established in certain groups of patients: it improves oxygenation (but not survival) in patients with acute respiratory distress syndrome(1), and it is used in neonatology for management of persistent pulmonary hypertension of the newborn(2). But it can be applied in other resuscitation settings: in arrested or peri-arrest patients with pulmonary hypertension.
