This video shows the mechanism for dislodgement and deformation of humeral intraosseous needles and how to avoid this.
In summary, if you need to abduct the arm (eg. for thoracostomy), keep the thumbs down (ie. have the arm internally rotated at the shoulder). Otherwise the IO catheter may bend or fall out.
Occasionally we step out of the resuscitation room feeling like a case should have gone better, but it can be hard to put our finger on just where it went wrong. In my last post I discussed the STEPS approach to analysing resuscitation cases: Self, Team, Environment, Patient and System.
Occasionally you can get a case where the STEPS seem to be aligned but things still feel bad. In which the outcome was unsatisfactory because the plan was wrong, or the team wasn’t able to execute the plan. Consider the following case.
1. A patient with a past history of DVT no longer on anticoagulants presents with chest pain and syncope.
She is severely hypotensive with a raised jugular venous pressure and a clear chest x-ray. A working diagnosis of pulmomary embolism is made.
Discussions ensue regarding empirical fibrinolysis and a respiratory physician is consulted, who over the phone cautions against treating without a CT pulmonary angiogram.
The patient is given heparin and transferred to the CT scanner where she arrests. Intravenous rtPA is given during CPR but no return of spontaneous circulation is achieved and she is pronounced dead after 30 minutes of resuscitation.
On this occasion the team worked efficiently and communicated well under clear leadership. Everyone knew the plan and shared the mental model. The environment was well controlled and the patient had been swiftly moved to CT within 20 minutes of arrival. Thanks to simulation training the well rehearsed cardiac arrest resuscitation was conducted with precision and the team was able to rapidly access the thrombolytic and knew the correct dose.
By a quick STEPS analysis, this case appears to have gone as well as could be expected. Perhaps there is nothing to learn. Some you win, some you lose, no?
No. Autopsy revealed type A aortic dissection with pericardial tamponade.
The management may have been efficient but it failed to be effective. In other words, things were done right, but the right things weren’t done; they did the wrong things right.
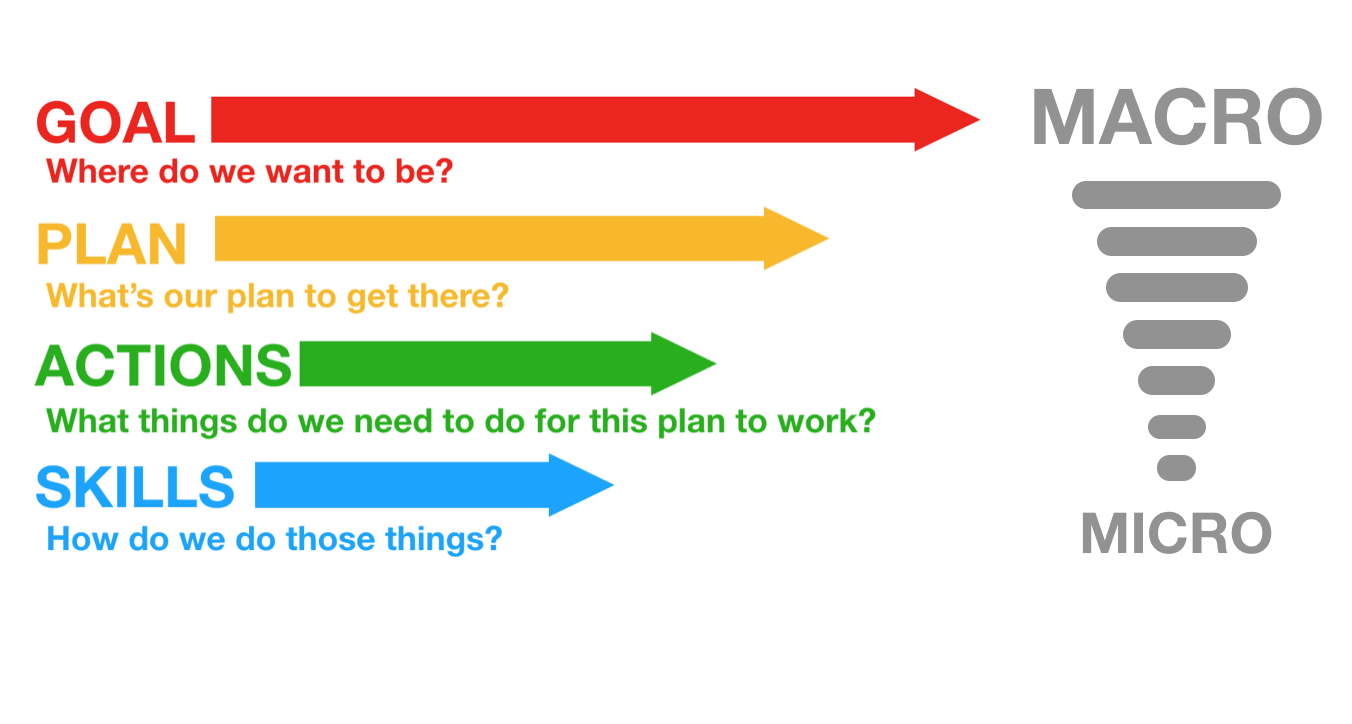
This might be an example where STEPS is inadequate, and instead we should evaluate the clinical trajectory. The cognitive bias that led to a lack of consideration of alternative diagnoses might be classifiable under ‘self’ or ‘team’ but I find it more helpful to consider it under a failure of strategy. What is strategy? Strategy in my mind is another word for plan. The plan is based on a particular resuscitation goal, and will consist of the procedures & skills required to action the plan. We can thus break down an attempted clinical trajectory into:
Goal (what are we trying to achieve) Strategy, or Plan (what’s our plan to get there?) Tactics, or Actions (what procedures will be required to execute the plan) And, at more granular level: If we’re failing at the procedural level, the components of procedures, namely Skills & Microskills. So, as we zoom in from macro to micro in setting the clinical trajectory, we can look at Goals, Plan, Actions, and Skills: In the above case it appears the following was applied, in terms of Goal-Plan-Actions-Skills:
G – resuscitate hypotensive patient P – give fibrinolysis for likely PE A – consult respiratory physician, get CTPA S – request scan, give heparin, transport to CT
The goal was appropriate, but the plan was ineffective.
The following approach would have been more effective.
G – resuscitate hypotensive patient P – identify cause of undifferentiated hypotension and initiate treatment in the resus room A – thorough bedside assessment in patient too sick to move: history, physical, CXR, ECG, labs, POCUS S – Basic cardiac ultrasound
By planning to identify and treat the cause of hypotension in the resus room, the more appropriate investigation would have been selected (cardiac ultrasound) and the correct diagnosis is much more likely to have been made.
Let’s look at some other cases:
2. An 88-year-old male presents by ambulance to the ED with dizziness. He is hypotensive, pyrexial, hypoxic and confused.
His chest x-ray shows likely bronchopneumonia. He has appropriate initial resuscitation and ICU is consulted. Soon he is intubated and on high dose vasoactive medication with escalating doses despite ongoing hypotension, anuria, and a lactate of 11 mmol/l, increased from 8 on arrival.
As he is being wheeled off down the corridor towards ICU his distraught and frail wife arrives. She is taken to the quiet room where she explains that her husband would never want to be ‘on a life support machine’ and asks ‘can’t you just keep him comfortable’?
G – the goal – to provide maximally aggressive resuscitation – was not in keeping with the patient’s wishes. If the goal had been to provide care in accordance with his wishes, the plan could have included attempts to ascertain these sooner while providing initial treatment. Upon gaining sufficient information, a new goal can be established: maximising the patient’s comfort and dignity.
3. An obese 30-year-old female presents with syncope. At triage she is pale, tachycardic & hypotensive. Clinical and sonographic assessment, including free intraperitoneal fluid and a positive urine HCG, is suggestive of ruptured ectopic pregnancy.
The gynaecologist and anaesthetist ask the ED team to bring the patient straight to the operating room. The ED team spends 20 minutes struggling to obtain intravenous access, eventually placing a 22G intravenous catheter in the patient’s hand and a humeral intraosseous needle.
Her shock is considerably worse on arrival in theatre, despite attempts to transfuse O negative blood en route.
Goal – get her safely to the operating room Plan – vascular access, cross match blood, start haemostatic resuscitation, go to OR as soon as possible Actions – peripheral and/or intraosseous cannulation attempts Skills – vascular access skills
Here the failure was at the actions and skills level. Better vascular access could have been attained using ultrasound guided peripheral cannulation, or central vascular access, or earlier intraosseous insertion.
4. A 120kg 32-year-old male with a history of deliberate self harm presents on the night shift with coma due to mixed benzodiazepine and venlafaxine overdose.
The decision is made to intubate for airway protection. After rapid sequence induction direct laryngoscopy is attempted by the emergency registrar who obtains a grade 4 view. Cricoid pressure is removed resulting in a grade 3 view.
The registrar asks for a bougie which she passes and then railroads the tracheal tube over it. The cuff is inflated, capnography is connected, and the self-inflating bag is connected and squeezed while the chest is auscultated.
The abdomen distends, the capnograph remains flat, and gastric contents are seen to pass upward through the tube into the self-inflating bag. The tube is immediately removed and bag-mask ventilation is attempted. The oxygen saturation is now 78% and the airway is soiled. The airway is suctioned and repeat attempts to bag-mask ventilate fail. A successful cricothyroidotomy is performed and the patient subsequent has full neurological recovery.
Goal – Provide supportive care and minimise complications from overdose Plan – Airway protection and admit to ICU for monitoring Actions – Rapid sequence intubation, ICU referral Skills – Pre-, peri- and post-intubation oxygenation techniques; patient positioning; rapid sequence induction of anaesthesia; direct laryngoscopy; bougie handling techniques; external laryngeal manipulation
In this case the patient was not placed in the ramped position and no nasal cannulae were applied for apnoeic oxygenation. A tube was railroaded over an oesophageal bougie, which arguably should not occur if ‘hold up’ is sought when the bougie is placed.
Although the goal, plan and actions were appropriate, the team did not demonstrate adequate skill in this procedure. Likely due to a failure of training, standardised procedures, and checklists (or their application), this could also be identified as a ‘system’ problem in STEPS. It is also possible that the intubator forgot her training under stress – a problem classifiable under ‘self’. Alternatively other members of the team may have had knowledge but didn’t speak up or cross-check their colleague, which would be a ‘team’ issue.
Limitations of this approach This sort of analysis is retrospective and subjective and at risk of hindsight bias (e.g. distortion due to projection, denial, or selective recall). However, these limitations do not negate the value of the learning exercise, particularly if we are aware of them and strive to minimise their impact (e.g. write down the details of a cases as soon as possible afterward). It at least provides a structure for individuals and teams to begin the conversation about where and how things may have been suboptimal.
Goals may be multiple and may change according to incoming information, and for each goal there may be several viable alternative plans. STEPS and GPAS may overlap, eg. team failures may result in inappropriate goals and strategies, or in failed procedures.
Summary These models may prove helpful as a means of dissecting a case in a structured way. Put simply, STEPS offers a structure for identifying efficiency improvements (“doing things right”) and GPAS can help us assess effectiveness (“doing the right things”).
Another way of looking at it is that STEPS provides the components of a resus at any point in time, and GPAS defines the trajectory: where the resus is going and how to get there.
I use this structure to analyse cases in my own clinical practice and in my teaching. I would be interested to hear from others’ experience. Do you find this approach useful in identifying areas for improvement in those cases that you feel should have gone better?
Thanks to Chris Nickson for his comments and improvements to this post
A resuscitationist agonises. These words, expressed by Scott Weingart during a podcast we did together, ring true to all of us who strive to improve our practice. Driven by the passionate conviction that we should never lose a salvageable patient through imperfect care, we relive cases and re-run them through our mental simulators to identify areas for improvement.
In the search for actionable items though, we occasionally exit this process empty-handed. Something about a case felt wrong although ostensibly all the clinical interventions may have been appropriate. It is in these cases that it can be helpful to have a structure to aid analysis.
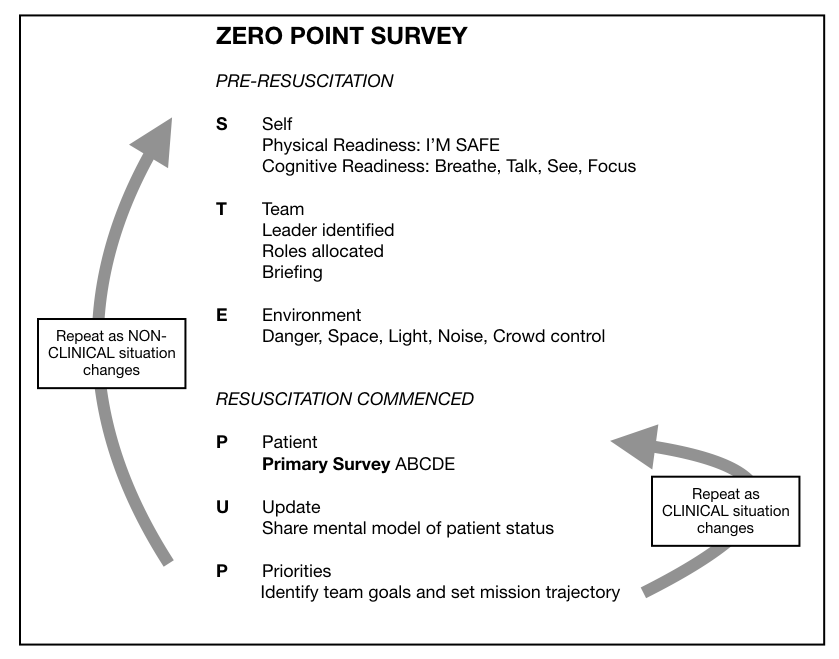
I, along with an international, interdisciplinary faculty of resuscitationists, have previously proposed an easily remembered system for optimising the clinical and non-technical components of resuscitation immediately before and during a patient encounter, dubbed the ‘Zero Point Survey’ (ZPS)(1), so called because first contact with a patient is rarely ‘Time Zero’ for a prehospital mission or hospital resuscitation case; there is invariably time for preparation of oneself, one’s team, and the environment (including equipment) prior to the primary survey and commencement of resuscitation. Following the assessment and management of STEP (self, team, environment & patient), the team should be regularly Updated on patient status and informed of the Priorities.
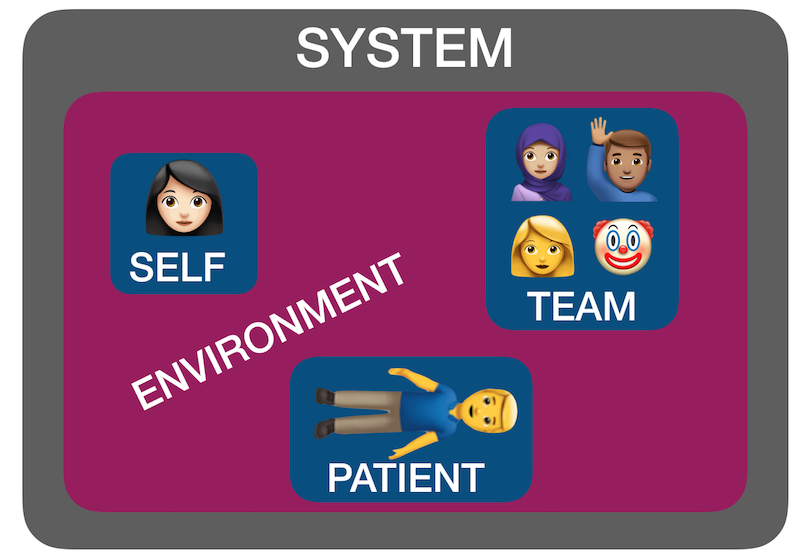
But ‘self, team, environment and patient’ isn’t just a useful system for case preparation. It can also be used for case analysis. I have found by discussing many ‘unsatisfactory’ cases over the years with participants in human factors workshops that STEP can help us identify where the issues lie. Accompanying all these factors is another ’S’: the system in which they interplay – the organisational rules, processes, policies, resources and deficiencies that may facilitate or obstruct an effective resuscitation(2).
Using STEPS to analyse cases The following (genuinely) hypothetical resus cases demonstrate how the application of this framework – Self, Team, Environment, Patient, System – might help identify correctible factors for future resuscitations:
1. Cardiac arrest in the bathroom on the orthopaedic ward – “it was chaos, there were too many people, and the resus trolley wasn’t properly stocked”.
STEPS analysis: Team – Leader needed to assign roles and allocate tasks Environment – Crowd control needed, lack of equipment System – Adequate checks for resus trolley not in place
2. 19-year-old male stabbed in the chest and arrested on arrival in hospital. CPR provided but went from PEA to asystole. Team leader discontinued resus after 20 minutes. Resident: “I thought he needed a resuscitative thoracotomy but no-one was willing to do it. No-one even mentioned it”.
STEPS analysis: Self – Lacked confidence to speak up, doubted own knowledge or influence Team – Lack of team situational awareness or knowledge or skill regarding required intervention System – Insufficient training and preparation for penetrating traumatic cardiac arrest scenario
3. 30-year-old mother with abdominal wound and her 2-year-old daughter with massive open head injury, both due to gunshot wounds, having been shot by husband/father who killed himself on scene. Child arrests in the ED, without ROSC, witnessed by mother before mother is taken to operating theatre.
STEPS analysis: Patient(s) – tragic case with upsetting circumstances and compounded psychological distress for patient and staff. The best resuscitation team in the world is not going to feel good about this one.
4. 46-year-old previously healthy male with VF arrest achieved ROSC after prehospital defibrillation and brought to the ED of a non-cardiac centre comatose and intubated. Further refractory VF in ED. Received multiple shocks, antiarrhythmics, double sequential external defibrillation. No on-site access to mechanical CPR, cardiac catheterisation, or ECMO. Patient declared dead in ED.
STEPS analysis: System – Prehospital team gave excellent care but brought the patient to a hospital ill-equipped to manage his ongoing needs, due to lack of ambulance service policy regarding appropriate destination hospital for cardiac arrest cases.
Summary You can see from the above cases how STEPS may be applied to make some sense of where a resus has gone wrong. Note that I am not recommending this as a way of structuring a team debrief or formal incident investigation – many institutions already have processes for conducting these and various rules and sensitivities have to be accommodated. Rather, this is a format I’ve found helpful in applying during informal discussions that aim to get the nub of where things could or should have gone better.
Occasionally, you can get a case where the STEPS seem to be aligned but things still feel bad – in which the outcome was unsatisfactory because the plan was wrong, or the team wasn’t able to execute the plan. In my next post I’ll discuss another way of analysing cases that can accompany STEPS.
This is a guest post from Dr Per Bredmose, anaesthetist and retrieval medicine physician in Norway, also known as Viking One
I struggle to ventilate the patient in the resus room, airway pressures are high, the bag doesn’t empty properly. In my mind I plan ahead for the next step. Through my mind goes the thought – is this the one, the one that I cannot ventilate? Statistically it is not likely to be, but I am prepared to add two-person technique, airway adjuncts like nasopharyngeal or oropharyngeal, or supraglottic devices that I use frequently in theatre. I feel confident in the use of these methods, and (in the worst case) in cricothyroidotomy. I have practiced that numerous times on our live-tissue course on anaesthetised pigs. However – before I start any of these actions.. I routinely, almost as a reflex from theatre turn the patient’s head 45 degrees to the left, and then the bag suddenly empties easily – and I can ventilate the patient.
Some people think that time with TIVA in theatre has little value for emergency medicine and advanced prehospital care. I strongly disagree. This is some of the most relevant and valuable time I have for keeping and optimising my practical skills. Bag-valve-mask (BVM) ventilation is an essential core skill for any prehospital provider. In theatre this manoeuvre is well known and frequently practiced. It is my impression that this head rotation is less used, and even maybe less well known outside theatre, and especially in the prehospital field. Therefore this is a reminder of an old technique.
When to do it: When encountering difficulties in conventional BVM ventilation, either when you cannot ventilate or when it’s just difficult to ventilate.
How to do it: Keep a firm one hand grip and gently rotate the head 45 degrees towards the side of the hand with the jaw grip. At the same time, one can try to optimise the one-hand-jaw thrust that goes along with BVM ventilation. Occasionally one needs to extend (dorsiflex) the neck a bit further to fully open the airway. The technique can also be used as a two-person technique, although this is rarely needed.
Opposition: Frequently I hear that I cannot transfer practice from theatre to the prehospital field. Well, this seems to work well in theatre, in ICU and in the field – airways are airways!!
Recently an article in European Journal of Anaesthesiology by Itagaki et al(1) with a cross over design showed an increase in tidal volume when the patients were ventilated in a head rotated position compared to neutral position with the same airway pressure. Their conclusion was as follows: Head rotation of 45° in anaesthetised apnoeic adults significantly increases the efficiency of mask ventilation compared with the neutral head position. Head rotation is an effective alternative to improve mask ventilation if airway obstruction is encountered. Therefore – this is a useful tool that one always should have in the “practical toolbox”. It is not always the solution, but occasionally it saves you (and the patient) a lot of trouble.
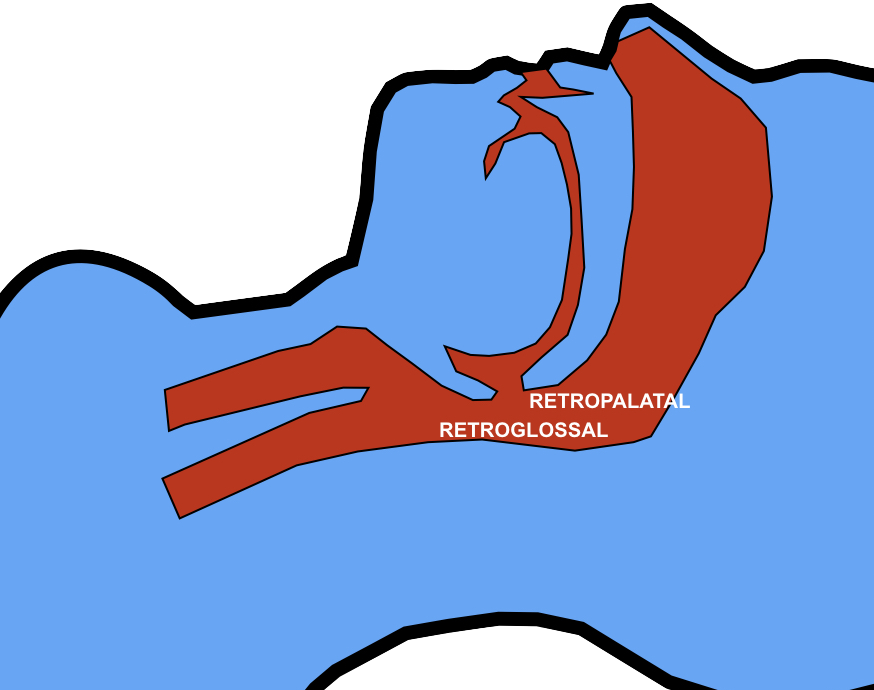
Thoughts from Dr Cliff Reid I haven’t used this approach and wasn’t aware of previous research showing an increase in the retroglossal (but not retropalatine) spaces in (awake) patients with head rotation(2).
The mechanism is thought to be gravitational. It is also possible that neck rotation increases upper airway wall tension that reduces collapsibility of the lumen.
In this elegantly designed new study, a two handed BMV technique was used, similar to that advocated in my prehospital & emergency medicine environments. The rotation was always to the right, although the authors comment that they would expect the same results on the left. The increased tidal volume effect with head rotation occurred mostly in younger patients and patients with Mallampati classification I. Such patients are unlikely to be difficult to mask-ventilate, limiting the applicability of these findings to patients who are difficult to ventilate. However having one more option to employ to improve BMV efficacy (after two person technique, optimising ear-to-sternal-notch positioning, and inserting oro- and/or nasopharyngeal airways) may be useful, and the experience and perspective of my anaesthetic colleague Viking One is definitely food for thought. Obviously one should avoid this if there is potential neck injury so I won’t be trying it my trauma patients.
1. Itagaki T, Oto J, Burns SM, Jiang Y, Kacmarek RM, Mountjoy JR. The effect of head rotation on efficiency of face mask ventilation in anaesthetised apnoeic adults. Eur J Anaesthesiol. 2017 Jul;34(7):432–40.
2. Ono T, Otsuka R, Kuroda T, Honda E, Sasaki T. Effects of head and body position on two- and three-dimensional configurations of the upper airway. J Dent Res. 2000 Nov;79(11):1879–84.
An engaging scene from ‘Code Blue‘ demonstrated a Helicopter Emergency Medical Service team managing a patient with major thoracic haemorrhage. They did a right thoracotomy and wanted to clamp the hilum but there was some kit missing from the pack.
Unfortunately, the video is no longer available.
This scene had some great discussion points for prehospital professionals, even if the specific scenario is somewhat unlikely for most people’s practice:
Non-compressible haemorrhage is possibly the biggest single clinical challenge when you’re a long way from hospital
Agitated friends and family can be disruptive – allocate a rescuer to look after them
Having blood products to give is essential
Don’t rely on the memory of individuals, who are fallible, to pack your equipment. “I was sure I put them in” didn’t cut it when the team needed forceps to clamp the pulmonary hilum and stop the bleeding. Checklists are the in thing, for good reason.
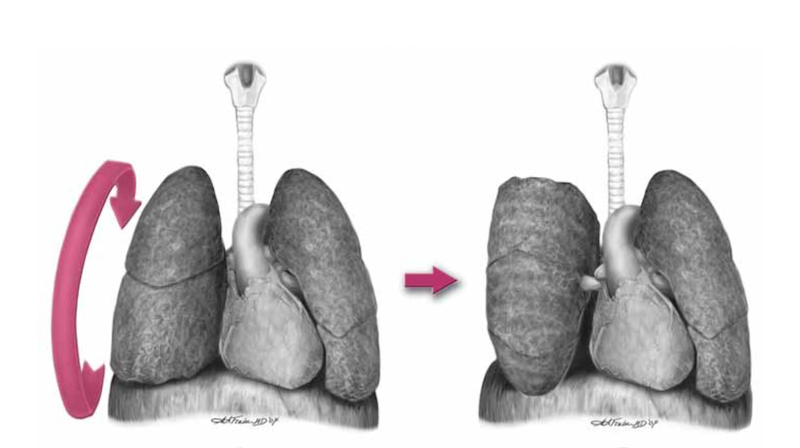
Luckily, you don’t need to clamp the hilum (which is tricky) in massive unilateral thoracic haemorrhage. You can just twist the lung 180 degrees on the hilum so it’s upside down. This can prevent further haemorrhage and air embolism.
What’s a hilar twist then?
The hilar twist manoeuvre, as it’s called, is worth learning if you’re a clinician who is prepared to do resuscitative clamshell thoracotomy for penetrating traumatic cardiac arrest. The clamshell is quick and provides excellent exposure(1) and is preferred to lateral thoracotomy(2).
The primary purpose of clamshell thoracotomy in penetrating traumatic arrest is to relieve cardiac tamponade and control a cardiac wound(3). It is well described and continues to save lives in the prehospital setting(4).
However, sometimes you’ll open the chest and the pericardium will be empty (other than containing the heart of course), and there will be massive haemorrhage on one side of the chest. Although most of these patients will be unsalvageable outside a trauma centre’s operating room, it’s worth trying something once you’ve gone to all the trouble of opening the chest. The hilar twist(5) is probably the best option for the non-surgeon, especially when some muppet’s forgotten to pack a clamp.
In order to make the lung mobile enough to twist, it’s first necessary to cut through the inferior pulmonary ligament. This is also known as simply the pulmonary ligament (because there’s no superior equivalent) and sometimes the inferior hilar ligament. It’s not actually a ligament, but an extension of the parietal pleura extending downwards in a fold from the hilum. Some describe it as hanging down from the hilum like a ‘wizard’s sleeve’, which invariably gets a giggle from some of our trainees from the United Kingdom for some reason.
After cutting the ligament completely to the level of the inferior pulmonary vein, the lung is then twisted ‘lower lobe towards you’, ie. lower lobe is rotated anteriorly over the upper lobe until the lung is oriented ‘upside down’. The twisted vessels around the hilum become occluded and further haemorrhage from that side should be limited. Other priorities in the arrested patient will be aortic occlusion, internal cardiac massage, and blood products. Packs may be required to keep the lung from untwisting, and if return of spontaneous circulation is achieved, there is a risk of dysrhythmia, right heart failure, and refractory hypoxaemia.
I’ve only done this on pigs and human cadavers so am not speaking from any reassuring level of experience or competence. The literature is out there to read, and it’s up to you to decide how you want to expand or limit your options when you’ve cracked that chest in an arrested patient.
References
1. Flaris AN, Simms ER, Prat N, Reynard F, Caillot J-L, Voiglio EJ. Clamshell incision versus left anterolateral thoracotomy. Which one is faster when performing a resuscitative thoracotomy? The tortoise and the hare revisited. World J Surg. 2015 May;39(5):1306–11.
2. Simms ER, Flaris AN, Franchino X, Thomas MS, Caillot J-L, Voiglio EJ. Bilateral Anterior Thoracotomy (Clamshell Incision) Is the Ideal Emergency Thoracotomy Incision: An Anatomic Study. World J Surg. 2013 Feb 23;37(6):1277–85.
The London Trauma Conference remains up there on my list of ‘must go’ conferences to attend. It marks the end of the year, fills me with hope and inspires me for the future. Unfortunately this year I was torn between the conference and the demands of clinical directorship so I could only get to the “Air Ambulance & Prehospital Care Day”. At least this way I’m saved from the dilemma of which sessions to attend!
So what were the highlights of the Prehospital Day? For me, they were Prehospital ECMO,’Picking Up the Pieces’, and the REBOA update. Prehospital ECMO Professor Pierre Carli gave us an update on prehospital ECMO. Professor Carli (not to be confused with the equally awesome Professor Carley) is the medical director of Service d’Aide Médicale Urgente (SAMU) in Paris. They’ve been doing prehospital ECMO in Paris since 2011 and the data analysed over three years reveals a 10% survival to hospital discharge rate. We know from the work in Asia that successful outcome following traditional cardiac arrest management and ECPR is related to the speed of the intervention. Transposing the time to intervention from his 2011 – 2013 data onto the survival curve that Chen et al produced explains why the success rate is limited:
The revised 2015 process aims to reduce the duration of CPR, reduce time to ECMO and therefore improve survival to discharge rates. They are doing this by dispatching the ECMO team earlier.
The eligibility criteria for ECPR is also changing; patients >18 and <75years, refractory cardiac arrest (defined as failure of ROSC after 20min of CPR), no flow for < 5 minutes with shockable rhythm or signs of life or hypothermia or intoxication, EtCO2 > 10mmHg at time of inclusion and no major comorbidity.
Already there appears to be an improvement with 16 patients treated using the revised protocol with 5 survivors (31%) – although we must be wary of the small numbers.
A concern that was expressed by the French Department of Health was the fear of a reduction in organ donation with the introduction of ECPR – it turns out that rates have remained stable. In fact the condition of non heart beating donated organs is better when ECMO has been instigated; the long term effects on organ donation are being assessed.
I’m without doubt that prehospital ECMO/ED ECMO is the future although currently in the UK our hospital systems aren’t ready for this. If you want to learn more then look at the ED ECMO site or book on one of the many emerging courses on ED ECMO including the one that is run by Dr Simon Finney at the London Trauma Conference, or if you want to go further afield you could try San Diego (although places are fully booked on the next course). Picking Up the Pieces
The Keynote speaker was Professor Sir Simon Wessely. He is a psychiatrist with a specialist interest in military psychology and his brief was to describe to us the public response to traumatic incidents. He has worked with the military and in civilian situations. After the 7/7 London bombings the population of London was surveyed: those most likely to be affected were of lower social class, of Muslim faith, those that had a relative that was injured, those unsure of the safety of others, those with no previous experience of terrorism and those experiencing difficulty in contacting others by mobile phone. Obviously there are many factors that we cannot influence however on the basis of the last risk factor our response to incidents has changed – the active discouragement to make phone calls has been changed to a recommendation of making short calls to friends and relatives.
The previous practice of offering immediate psychological debriefing to those involved in incidents was discounted by Prof Wessely – his research demonstrated that this intervention was not only not required but could actually result in harm: only a minority have ongoing psychological distress that can benefit from formal psychological input, which should occur later.
The approach that should be taken is to allow that individual to utilise their own social networks (family, friends, and colleagues) and to accept that in some cases the individual may not want or need to talk. This has led to the development of the Trauma Risk Management (TRIM) system which provides individuals within organisations that are exposed to traumatic events the skills required to identify those at risk of developing psychological problems and to recognise the signs and symptoms of those in difficulty. To a certain extent we naturally do this for our peers – I have spent many a night sitting in the ‘Good Samaritan’ pub with colleagues from the Royal London Hospital and London’s Air Ambulance – but having a more formal system is probably of benefit to enable those who have ongoing difficulties to access additional support. REBOA update
Finally, the REBOA update – Resuscitative Endovascular Balloon Occlusion of the Aorta. One year on, Dr Sammy Sadek informed us that there are now more courses teaching the REBOA technique than there are (prehospital) patients that have received it. Over the last year only seven patients have qualified for this intervention in London, far fewer than they had anticipated. Another three patients died before REBOA could be instigated. All patients had a positive cardiovascular response. Four of the seven died from causes other than exsanguination. Is it worth all the effort and resource to deliver this intervention when such a select group will benefit?
Obviously there was much more covered in the day, this is just a taste. If you’ve never been to the London Trauma Conference then I definitely would recommend it and even if you have been before there are so many breakout sessions now there is always something for everyone. More on the London Trauma Conference:
Keep an eye on the LTC website for information on the 2016 conference.
The critical care and #FOAMed community lost our friend Dr John Hinds a few days ago.
We’re in the business of sudden death. As prehospital, emergency, acute medicine and intensive care clinicians, facing the reality of the tragic loss of a living person, loved by their friends and family, is our day job. This makes me think we shouldn’t really have any reason to be ‘shocked’ or ‘surprised’. But we have every right to be sad.
The news came in the same week as the tragic Flight for Life Helicopter Crash in Colorado, bringing us another unwelcome reminder of the dangers of prehospital work. My HEMS colleagues and I are always mindful of the possibility that every time we get in the helicopter it could be our last, and I’ve no doubt John appreciated this reality when responding on his motorcycle.
I admired John as he was the quintessential resuscitationist. He was not bound by specialty or location in his passion for excellence in life-saving medicine. He was a master (and innovator) of advanced prehospital emergency medicine in a region where it still barely exists. He was supportive of emergency physicians providing emergency anaesthesia. He performed the first thoracotomy for more than a decade in one hospital, prompting a review of systems, equipment and training and bringing specialties together to embrace multidisciplinary trauma management. He inspired our friends across the world with his approach to intensive care patients.
Two weeks ago John and I gave two of the opening talks at the SMACC conference in Chicago. My talk went first – entitled ‘Advice to a Young Resuscitationist’. I attempted to list a number of tips that could help a resuscitationist become more effective at saving lives while surviving and thriving in our often traumatic milieu. The talk will be uploaded soon, and I’ve listed the pieces of advice below. What strikes me now like a slap across the face with a large wet fish is the realisation that John exemplified every one of these characteristics and habits:
1. Carve your own path that takes you on a richer path than that worn by trainees in a single specialty
John was an anaesthetist, an intensivist, and prehospital doctor.
2. Never waste an opportunity to learn from other clinicians – leave your ego at the door. See any feedback as an opportunity to learn and to improve, no matter how painful it is to receive.
Despite being among the best in his field, John would on occasion discuss challenging cases and ask if we could think of anything else that should have been done (our answer being, without exception, “no”).
3. Have the confidence and self-belief to perform actions you are competent to perform when needed, to avoid the tragedy of acts of omission.
John’s amazing talk on “crack the chest – get crucified” (when no-one else would) shows how he embraced this mindset: do what needs to be done – with honourable intentions – and manage the consequences later.
4. You can’t save every one, but you can make each case count. When a case goes wrong you need to change something – yourself, your colleagues or the system.
John was a super-agent of change wherever he operated. One beautiful example is how in one hospital the thoracotomy tray ended up being named after him!
5. Caring is so critical to what we do, and is one of the most important things to patients and their families.
As Greg Henry taught me (quoting Theodore Roosevelt) : ‘Nobody cares how much you know until they know how much you care’
John was gentle, kind, and humble. So many of his tributes remark on his compassion and dedication to patients.
6. Choose your colleagues & your environment well. Greater team cohesiveness is protective against burnout and compassion fatigue.
John was proud of the teamwork he enjoyed with his ICU colleagues, and worked with forward thinking colleagues who contribute significantly to #FOAMed.
7. Strive for balance in your life and your work. Consider part time working or mixing your critical care with a non-clinical or non-critical care interest.
John was revered and loved within the world of motorcycle racing, a passion he managed to combine with his flair for critical care.
8. Train your brain to be aware of and to utilise strategies that protect it against cognitive traps and avoidable performance limitations under stress – learn the hacks for your MINDWARE.
Many of us now introduce stressors into our simulation training to help us learn to deal with the adrenal load of a difficult resuscitation. But I doubt many of us can hope to achieve the intense focus and concentration under pressure that is required of motorcycle racers. John sent me a link to this video of racer Michael Dunlop a few weeks ago with the comment ‘How about this for a scare!’
9. Maintain perspective. It’s not all about you or your resus room.The most effective resuscitationists save lives when they’re not there. They work on the systems – the processes, the training, the governance, the audit, the research.
John was a brilliant educator and systems thinker. The care given at the roadside, in the ED, the ICU and the operating room at many sites is better because of the teaching he gave and the approaches he developed.
10. Understand that everything you say and do in a resuscitation casts memorable impressions in trainees’ minds like the tossing of pebbles into a pond, whose ripples reach out and out to affect so many future lives and deaths in other resuscitation rooms.
You can imagine the obstacles and personalities John faced when trying to improve care in the environments in which he worked. But through it all he remained a gentleman. Always constructive, always collaborative, always supportive. I’ve never heard him say a bad word about any named individual or criticise another specialty. He truly embodied the non-tribal spirit of SMACC, which sets an example for us all to aspire to, and will influence future resuscitation room behaviour in far-reaching locations.
11. Behave as you would want to be remembered, and be mindful of the extent of the ripples in the pond. But don’t let that put you off throwing the pebbles – embrace the challenge of the highs and lows and above all enjoy the ride, for it is awesome.
In just 35 years of life John saved the lives of many and changed the lives of many more. He knew how to throw pebbles and wasn’t afraid to point out the lack of emperor’s clothes around many traditional aspects of medical practice. And that smile seen in all the pictures of him shows there’s no doubt John enjoyed the ride, and it was awesome. Thanks to his wit, intelligence, teaching, charm, and resuscitation brilliance, he helped us enjoy it all the more too.
I spent a lot of time preparing my talk ‘Advice to a Young Resuscitationist’. It’s clear to me now that I needn’t have bothered. Sharing the stage with John, I could have saved everyone’s time by simply saying: ‘Try to be like THIS guy’.
I am extremely privileged to know him, to have learned from him, and to have shared some moments from his days at smaccUS.
We will mourn, we will remember, and we will honour him by being the best resuscitationists we can.
You can also honour him by signing the Northern Ireland Air Ambulance petition
Many clinicians extrapolate adult research findings to paediatric patients because there’s no alternative, and until now we’ve had to do that with post-cardiac arrest therapeutic hypothermia after paediatric cardiac arrest.
However the THAPCA trial in the New England Journal of Medicine now provides child-specific data.
It was a multicentre trial in the US which included children between 2 days and 18 years of age, who had had an out-of-hospital cardiac arrest and remained comatose after return of circulation. They were randomised to therapeutic hypothermia (target temperature, 33.0°C) or therapeutic normothermia (target temperature, 36.8°C) within 6 hours after the return of circulation.
Therapeutic hypothermia, as compared with therapeutic normothermia, did not confer a significant benefit with respect to survival with good functional outcome at 1 year, and survival at 12 months did not differ significantly between the treatment groups.
These findings are similar to the adult TTM trial, although there are some interesting differences. In the paediatric study, the duration of temperature control was longer (120 hrs vs 36 hrs in the adult study), respiratory conditions were the predominant cause of paediatric cardiac arrest (72%), and there were only 8% shockable rhythms in the paediatric patients, compared with 80% in the adult study.
The full text is available here. Therapeutic Hypothermia after Out-of-Hospital Cardiac Arrest in Children N Engl J Med. 2015 Apr 25
[EXPAND Abstract]
Background: Therapeutic hypothermia is recommended for comatose adults after witnessed out-of-hospital cardiac arrest, but data about this intervention in children are limited.
Methods: We conducted this trial of two targeted temperature interventions at 38 children’s hospitals involving children who remained unconscious after out-of-hospital cardiac arrest. Within 6 hours after the return of circulation, comatose patients who were older than 2 days and younger than 18 years of age were randomly assigned to therapeutic hypothermia (target temperature, 33.0°C) or therapeutic normothermia (target temperature, 36.8°C). The primary efficacy outcome, survival at 12 months after cardiac arrest with a Vineland Adaptive Behavior Scales, second edition (VABS-II), score of 70 or higher (on a scale from 20 to 160, with higher scores indicating better function), was evaluated among patients with a VABS-II score of at least 70 before cardiac arrest.
Results: A total of 295 patients underwent randomization. Among the 260 patients with data that could be evaluated and who had a VABS-II score of at least 70 before cardiac arrest, there was no significant difference in the primary outcome between the hypothermia group and the normothermia group (20% vs. 12%; relative likelihood, 1.54; 95% confidence interval [CI], 0.86 to 2.76; P=0.14). Among all the patients with data that could be evaluated, the change in the VABS-II score from baseline to 12 months was not significantly different (P=0.13) and 1-year survival was similar (38% in the hypothermia group vs. 29% in the normothermia group; relative likelihood, 1.29; 95% CI, 0.93 to 1.79; P=0.13). The groups had similar incidences of infection and serious arrhythmias, as well as similar use of blood products and 28-day mortality.
Conclusions: In comatose children who survived out-of-hospital cardiac arrest, therapeutic hypothermia, as compared with therapeutic normothermia, did not confer a significant benefit in survival with a good functional outcome at 1 year.
A key component in the planning of intubation is pre-oxygenation. Recently apnoeic oxygenation during laryngoscopy has been adopted too. These are just two components of an overall oxygenation strategy to consider when intubating the critically ill. Some patients will require proactive preparation of the components of successful post-intubation oxygenation, especially those with severe lung pathology like ARDS.
Here’s a handy list of things to consider when planning a peri-intubation oxygenation strategy. Some people like their airway stuff to begin with ‘P’, so I’ve obliged: