This video shows the mechanism for dislodgement and deformation of humeral intraosseous needles and how to avoid this.
In summary, if you need to abduct the arm (eg. for thoracostomy), keep the thumbs down (ie. have the arm internally rotated at the shoulder). Otherwise the IO catheter may bend or fall out.
This is a guest post from Dr Per Bredmose, anaesthetist and retrieval medicine physician in Norway, also known as Viking One
I struggle to ventilate the patient in the resus room, airway pressures are high, the bag doesn’t empty properly. In my mind I plan ahead for the next step. Through my mind goes the thought – is this the one, the one that I cannot ventilate? Statistically it is not likely to be, but I am prepared to add two-person technique, airway adjuncts like nasopharyngeal or oropharyngeal, or supraglottic devices that I use frequently in theatre. I feel confident in the use of these methods, and (in the worst case) in cricothyroidotomy. I have practiced that numerous times on our live-tissue course on anaesthetised pigs. However – before I start any of these actions.. I routinely, almost as a reflex from theatre turn the patient’s head 45 degrees to the left, and then the bag suddenly empties easily – and I can ventilate the patient.
Some people think that time with TIVA in theatre has little value for emergency medicine and advanced prehospital care. I strongly disagree. This is some of the most relevant and valuable time I have for keeping and optimising my practical skills. Bag-valve-mask (BVM) ventilation is an essential core skill for any prehospital provider. In theatre this manoeuvre is well known and frequently practiced. It is my impression that this head rotation is less used, and even maybe less well known outside theatre, and especially in the prehospital field. Therefore this is a reminder of an old technique.
When to do it: When encountering difficulties in conventional BVM ventilation, either when you cannot ventilate or when it’s just difficult to ventilate.
How to do it: Keep a firm one hand grip and gently rotate the head 45 degrees towards the side of the hand with the jaw grip. At the same time, one can try to optimise the one-hand-jaw thrust that goes along with BVM ventilation. Occasionally one needs to extend (dorsiflex) the neck a bit further to fully open the airway. The technique can also be used as a two-person technique, although this is rarely needed.
Opposition: Frequently I hear that I cannot transfer practice from theatre to the prehospital field. Well, this seems to work well in theatre, in ICU and in the field – airways are airways!!
Recently an article in European Journal of Anaesthesiology by Itagaki et al(1) with a cross over design showed an increase in tidal volume when the patients were ventilated in a head rotated position compared to neutral position with the same airway pressure. Their conclusion was as follows: Head rotation of 45° in anaesthetised apnoeic adults significantly increases the efficiency of mask ventilation compared with the neutral head position. Head rotation is an effective alternative to improve mask ventilation if airway obstruction is encountered. Therefore – this is a useful tool that one always should have in the “practical toolbox”. It is not always the solution, but occasionally it saves you (and the patient) a lot of trouble.
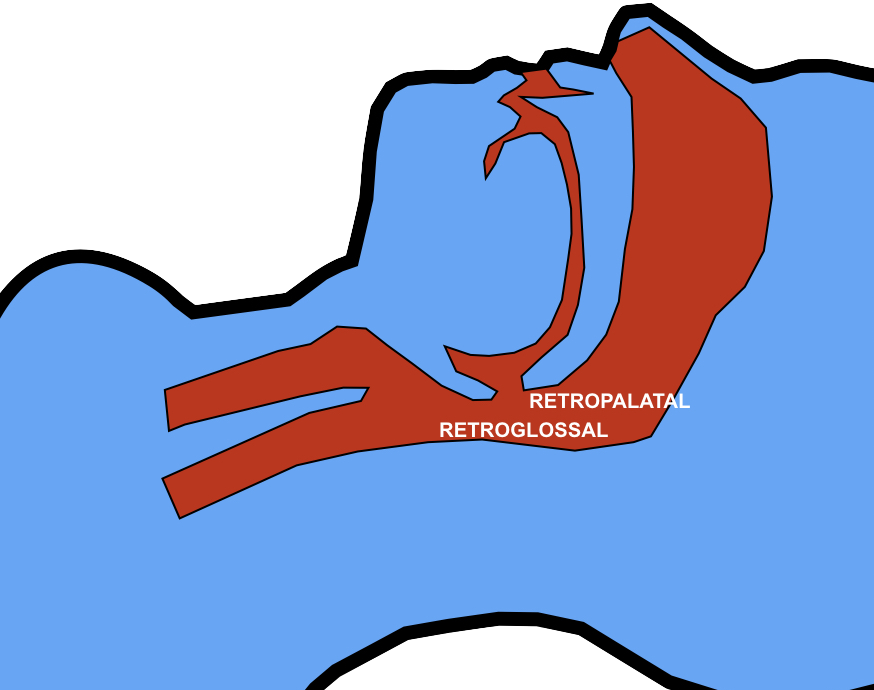
Thoughts from Dr Cliff Reid I haven’t used this approach and wasn’t aware of previous research showing an increase in the retroglossal (but not retropalatine) spaces in (awake) patients with head rotation(2).
The mechanism is thought to be gravitational. It is also possible that neck rotation increases upper airway wall tension that reduces collapsibility of the lumen.
In this elegantly designed new study, a two handed BMV technique was used, similar to that advocated in my prehospital & emergency medicine environments. The rotation was always to the right, although the authors comment that they would expect the same results on the left. The increased tidal volume effect with head rotation occurred mostly in younger patients and patients with Mallampati classification I. Such patients are unlikely to be difficult to mask-ventilate, limiting the applicability of these findings to patients who are difficult to ventilate. However having one more option to employ to improve BMV efficacy (after two person technique, optimising ear-to-sternal-notch positioning, and inserting oro- and/or nasopharyngeal airways) may be useful, and the experience and perspective of my anaesthetic colleague Viking One is definitely food for thought. Obviously one should avoid this if there is potential neck injury so I won’t be trying it my trauma patients.
1. Itagaki T, Oto J, Burns SM, Jiang Y, Kacmarek RM, Mountjoy JR. The effect of head rotation on efficiency of face mask ventilation in anaesthetised apnoeic adults. Eur J Anaesthesiol. 2017 Jul;34(7):432–40.
2. Ono T, Otsuka R, Kuroda T, Honda E, Sasaki T. Effects of head and body position on two- and three-dimensional configurations of the upper airway. J Dent Res. 2000 Nov;79(11):1879–84.
A key component in the planning of intubation is pre-oxygenation. Recently apnoeic oxygenation during laryngoscopy has been adopted too. These are just two components of an overall oxygenation strategy to consider when intubating the critically ill. Some patients will require proactive preparation of the components of successful post-intubation oxygenation, especially those with severe lung pathology like ARDS.
Here’s a handy list of things to consider when planning a peri-intubation oxygenation strategy. Some people like their airway stuff to begin with ‘P’, so I’ve obliged:
Some pectus excavatum patients have a metal ‘Nuss bar’ inserted below the sternum which can make chest compressions more difficult. In those without one, standard compression depths compress the left ventricle more than in non-pectus subjects, and might lead to myocardial injury.
This has led to a recommendation in the journal Resuscitation:
“Until further studies are available, we recommend strong chest compressions, according to the current guidelines, in PE patients with a sternal Nuss bar and, to minimize the risk of myocardial injury, we suggest a reduced chest compression depth (approximately 3–4 cm) at the level of lower half of the sternum in PE patients who have not had corrective surgery.”
Apnoeic oxygenation during laryngoscopy via nasal prongs has really taken off in the last couple of years in emergency department RSI, and is associated with decreased desaturation rates in out-of-hospital RSI.
More effective oxygenation and a small amount of PEEP can be provided by high flow nasal cannulae with humidified oxygen (HFNC)
A logical step in the progression of this topic is to consider HFNC for apnoeic oxygenation, and Reuben Strayer wrote about this nearly three years ago.
In a Twitter conversation today, Dr Pete Sherren highlighted a new article describing its use in anaesthesia for patients with difficult airways. This is labelled Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE). A reply from Dr Neil Brain points out that when used in kids, the bulkiness of the apparatus may get in the way of bag-mask ventilation (if that becomes necessary). But does HFNC apnoeic oxygenation confer any advantages over standard nasal cannulae?
In an apnoeic patient, 15l/min via standard cannulae should fill the pharyngeal space with 100% oxygen, and you can’t improve on 100%.
HFNC provide some continuous positive pressure, but this may be cancelled by the necessary mouth opening for laryngoscopy.
One issue with apnoea is of course a rise in carbon dioxide with consequent acidosis. The authors of the THRIVE paper (abstract below) point out that in previous apnoeic oxygenation studies, the rate of rise of carbon dioxide levels was between 0.35 and 0.45 kPa/min (2.7-3.4 mmHg/min), whereas with THRIVE the rise was 0.15 kPa/min (1.1 mmHg/min). They suggest that continuous insufflation with high flow oxygen facilitates oxygenation AND carbon dioxide clearance through gaseous mixing and flushing of the deadspace.
So should we switch from standard nasal cannula to high flow cannulae for apnoeic oxygenation? I think not routinely, but perhaps consider it in patients:
(1) with pressure-dependent oxygenation (eg. ARDS) although I’m not sure any CPAP effect would be sustained during laryngoscopy
and
(2) in patients with significant acidosis in whom a significant rise in carbon dioxide could be detrimental (eg. diabetic ketoacidosis).
I look forward to reading more studies on this, and to hearing from anyone with experience of this technique in the comments section. Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways. Anaesthesia. 2014 Nov 10. doi: 10.1111/anae.12923. [Epub ahead of print]
[EXPAND Abstract]
Emergency and difficult tracheal intubations are hazardous undertakings where successive laryngoscopy-hypoxaemia-re-oxygenation cycles can escalate to airway loss and the ‘can’t intubate, can’t ventilate’ scenario.
Between 2013 and 2014, we extended the apnoea times of 25 patients with difficult airways who were undergoing general anaesthesia for hypopharyngeal or laryngotracheal surgery. This was achieved through continuous delivery of transnasal high-flow humidified oxygen, initially to provide pre-oxygenation, and continuing as post-oxygenation during intravenous induction of anaesthesia and neuromuscular blockade until a definitive airway was secured. Apnoea time commenced at administration of neuromuscular blockade and ended with commencement of jet ventilation, positive-pressure ventilation or recommencement of spontaneous ventilation. During this time, upper airway patency was maintained with jaw-thrust.
Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE) was used in 15 males and 10 females. Mean (SD [range]) age at treatment was 49 (15 [25-81]) years. The median (IQR [range]) Mallampati grade was 3 (2-3 [2-4]) and direct laryngoscopy grade was 3 (3-3 [2-4]). There were 12 obese patients and nine patients were stridulous. The median (IQR [range]) apnoea time was 14 (9-19 [5-65]) min. No patient experienced arterial desaturation < 90%. Mean (SD [range]) post-apnoea end-tidal (and in four patients, arterial) carbon dioxide level was 7.8 (2.4 [4.9-15.3]) kPa. The rate of increase in end-tidal carbon dioxide was 0.15 kPa.min(-1) .
We conclude that THRIVE combines the benefits of ‘classical’ apnoeic oxygenation with continuous positive airway pressure and gaseous exchange through flow-dependent deadspace flushing. It has the potential to transform the practice of anaesthesia by changing the nature of securing a definitive airway in emergency and difficult intubations from a pressured stop-start process to a smooth and unhurried undertaking.
Patients in cardiac arrest due to severe hypothermia benefit from extracorporeal rewarming, and it is often recommended that they are treated at centres capable of providing cardiopulmonary bypass or extracorporeal membrane oxygenation (ECMO). But what if they’re brought to a centre that doesn’t have those facilities? If you work in such a centre do you have a plan, and are you familiar with what equipment you could use?
One option if you have an ICU is to provide extracorporeal warming using a haemofiltration machine used for renal replacement therapy(1). A double lumen haemofiltration catheter is inserted into a central vein and an ICU nurse can often do the rest, although some variables have to be set by the intensivist, often aided by a standard renal replacement therapy prescription chart. The machines are mobile and can be wheeled into the resus room (I have practiced this set up in resus). It might be worth discussing and practicing this option with your ICU.
Another extracorporeal option is to rig up a rapid infusion device such as a ‘Level 1’ to connect to arterial and venous catheters so that blood from the patient flows through and is warmed by the machine before being returned to the patient(2). Rapid rewarming has been achieved by this method but it requires some modification to the usual set up and so is much less likely to be a realistic option for most teams doing this on very rare occasions.
Less technical options are the traditionally taught warm saline lavage of body cavities such as the thorax and the peritoneal cavity. These can be achieved with readily available catheters and of course should be combined with ventilation with warmed gas and administration of warm intravenous fluid.
Thoracic lavage can be achieved with open thoracotomy or tube thoracostomy. One or two chest tubes can be placed on each side. One technique was described as:
Two 36 French chest tubes were placed in each hemithorax. One tube was placed in the fourth intercostal space in the mid-clavicular line. Another tube was placed into the sixth intercostal space in the mid-axillary line. Sterile saline at 39.0◦C was infused by gravity into each superior chest tube and allowed to drain passively through each inferior tube.(3)
Rapid rewarming at a rate of 6.8◦C per hour was achieved in an arrested hypothermic man using peritoneal lavage. It was done in the operating room with peritoneal lavage (saline 40◦C) with a rapid infusion system (Level 1) through two laparoscopic access sites. It was combined with external forced air rewarming and warm intravenous infusions(4).
Finally some devices manufactured for inducing hypothermia in post-cardiac arrest patients can also be used to rewarm patients, which might be endovascular devices, such as the Cool Line® catheter(5), or external, such as the Arctic Sun® Temperature Management System(6). It’s definitely worth finding out what your critical care services have as far as this equipment goes. In summary, although the ‘exam answer’ for cardiac arrest due to profound hypothermia is often ECMO/cardiopulmonary bypass, in most centres that’s not an option. It’s helpful to remind ourselves that (1) other extracorporeal rewarming options exist and (2) non-extracorporeal techniques can provide rapid rewarming.
1. Spooner K, Hassani A. Extracorporeal rewarming in a severely hypothermic patient using venovenous haemofiltration in the accident and emergency department. J Accid Emerg Med. 2000 Nov;17(6):422–4. Full text 2. Gentilello LM, Cobean RA, Offner PJ, Soderberg RW, Jurkovich GJ. Continuous arteriovenous rewarming: rapid reversal of hypothermia in critically ill patients. The Journal of Trauma: Injury, Infection, and Critical Care. 1992 Mar;32(3):316–25 PubMed 3. Plaisier BR. Thoracic lavage in accidental hypothermia with cardiac arrest — report of a case and review of the literature. Resuscitation. 2005 Jul;66(1):99–104. PubMed 4. Gruber E, Beikircher W, Pizzinini R, Marsoner H, Pörnbacher M, Brugger H, et al. Non-extracorporeal rewarming at a rate of 6.8°C per hour in a deeply hypothermic arrested patient. Resuscitation. 2014 Aug;85(8):e119–20. PubMed 5. Kiridume K, Hifumi T, Kawakita K, Okazaki T, Hamaya H, Shinohara N, et al. Clinical experience with an active intravascular rewarming technique for near-severe hypothermia associated with traumatic injury. Journal of Intensive Care. BioMed Central Ltd; 2014;2(1):11. link to abstract 6. Cocchi MN, Giberson B, Donnino MW. Rapid rewarming of hypothermic patient using arctic sun device. Journal of Intensive Care Medicine. 2012 Mar;27(2):128–30. PubMed
Are you someone who tries to determine whether an ECG trace is ‘irregularly irregular’ by drawing little dots on a piece of paper level with the R waves to see if they are evenly spaced? I’d done that for years until I read this fantastic suggestion, which I’ve been following for over a year now.
In the 1990s there was a popular series of posters and books called ‘Magic Eye‘. These contained a ‘random dot autostereogram‘ which appeared as a mish-mash of coloured dots, but when you stared at it for a while the illusion of a 3D image would emerge. They looked a bit like this (although this one won’t work at such reduced resolution):
Image Credit: Wikimedia Commons
Dr Broughton and colleagues from Cambridge, UK, discovered that this technique, which involves forcing a divergent gaze to get repeating patterns to appear to overlap, can be applied to an ECG trace.
Stereoviewing an ECG trace causes successive QRS complexes to visually overlap and produce a new image. As Broughton and colleagues point out:
“When achieved, this will lead to one of three outcomes. Entirely regular rhythms will ‘click’ into place as a new image at fixed depth. Rhythms with only mild irregularity may be stereoviewable, and if so, will appear to show successive QRS complexes at subtly varying depths. Rhythms with marked irregularity will not be stereoviewable, instead (in our experience) merely giving the viewer sore eyes after several failed viewing attempts.”
The authors assert that this can be applied to continuous ECG monitors, although unless you are really good at stereoviewing while moving your head/eyes horizontally, you should really freeze the trace on the screen first. The ‘Magic Eye®’ method of rhythm assessment Anaesthesia. 2012 Oct;67(10):1170-1
A recent study showed superior effectiveness of one bag-mask ventilation style over another in novice providers. The technique recommended is the thenar eminence grip, in which downward pressure is applied with the thenar eminences while the four fingers of each hand pull the jaw upwards toward the mask.
Interestingly, in their crossover study in which the thenar emininence (TE) technique was compared with the traditionally taught ‘CE’ technique, they demonstrated a ‘sequence effect’. If subjects did TE first, they maintained good tidal volumes when doing CE. However if they did CE first, they achieved poor tidal volumes which were markedly improved when switching to TE.
The authors suggest: “A possible explanation for this sequence effect is that the TE grip is superior. When one used the TE grip first, he or she was more likely to learn how a good tidal volume “feels” and then more likely to apply good technique with the EC grip.“.
Some of us have been practicing and teaching this technique for a while. None have put it better than the brilliant Reuben Strayer of EM Updates in this excellent short video:
STUDY OBJECTIVE: To determine which of two facemask grip techniques for two-person facemask ventilation was more effective in novice clinicians, the traditional E-C clamp (EC) grip or a thenar eminence (TE) technique.
SUBJECTS: 60 novice clinicians (medical and paramedic students).
MEASUREMENTS: Subjects were assigned to perform, in a random order, each of the two mask-grip techniques on consenting ASA physical status 1, 2, and 3 patients undergoing elective general anesthesia while the ventilator delivered a fixed 500 mL tidal volume (VT). In a crossover manner, subjects performed each facemask ventilation technique (EC and TE) for one minute (12 breaths/min). The primary outcome was the mean expired VT compared between techniques. As a secondary outcome, we examined mean peak inspiratory pressure (PIP).
MAIN RESULTS: The TE grip provided greater expired VT (379 mL vs 269 mL), with a mean difference of 110 mL (P < 0.0001; 95% CI: 65, 157). Using the EC grip first had an average VT improvement of 200 mL after crossover to the TE grip (95% CI: 134, 267). When the TE grip was used first, mean VTs were greater than for EC by 24 mL (95% CI: -25, 74). When considering only the first 12 breaths delivered (prior to crossover), the TE grip resulted in mean VTs of 339 mL vs 221 mL for the EC grip (P = 0.0128; 95% CI: 26, 209). There was no significant difference in PIP values using the two grips: the TE mean (SD) was 14.2 (7.0) cm H2O, and the EC mean (SD) was 13.5 (9.0) cm H2O (P = 0.49).
CONCLUSIONS: The TE facemask ventilation grip results in improved ventilation over the EC grip in the hands of novice providers.
An interesting animal study examined the techniques recommended in basic choking management algorithms for foreign body airway obstruction (chest and abdominal thrusts). In terms of the pressures generated, lateral chest thrusts were the most effective, although they are not recommended in current guidelines.
The technique described (on intubated pigs) was:
The animals were placed on the floor and on their side. The lower (dependent) side of the chest was braced by the ground and thrust was applied to the upper part of the upper side by two hands side by side with the higher one just below the axilla.
Interestingly – and I didn’t know this (although perhaps should have!) – the Australian Resuscitation Council (ARC) recommended lateral chest thrusts instead of abdominal thrusts for over 20 years.
While we should always exercise extreme caution in extrapolating animal studies to humans, this makes me want to consider lateral thrusts in the first aid (ie. no equipment) situation if other measures are failing. Lateral versus anterior thoracic thrusts in the generation of airway pressure in anaesthetised pigs Resuscitation. 2013 Apr;84(4):515-9
[EXPAND Abstract]
Objective Anterior chest thrusts (with the subject sitting or standing and thrusts applied to the lower sternum) are recommended by the Australian Resuscitation Council as part of the sequence for clearing upper airway obstruction by a foreign body. Lateral chest thrusts (with the victim lying on their side) are no longer recommended due to a lack of evidence. We compared anterior, lateral chest and abdominal thrusts in the generation of airway pressures using a suitable animal model.
Methods This was a repeated-measures, cross-over, clinical trial of eight anaesthetised, intubated, adult pigs. For each animal, ten trials of each technique were undertaken with the upper airway obstructed. A chest/abdominal pressure transducer, a pneumotachograph and an intra-oesophageal balloon catheter recorded chest/abdominal thrust, expiratory air flows, airway and intrapleural pressures, respectively.
Results The mean (SD) thrust pressures generated for the anterior, lateral and abdominal techniques were 120.9 (11.0), 135.2 (20.0), and 142.4 (27.3) cmH2O, respectively (p < 0.0001). The mean (SD) peak expiratory airway pressures were 6.5 (3.0), 18.0 (5.5) and 13.8 (6.7) cmH2O, respectively (p < 0.0001). The mean (SD) peak expiratory intrapleural pressures were 5.4 (2.7), 13.5 (6.2) and 10.3 (8.5) cmH2O, respectively (p < 0.0001). At autopsy, no rib, intra-abdominal or intra-thoracic injury was observed.
Conclusion Lateral chest and abdominal thrust techniques generated significantly greater airway and pleural pressures than the anterior thrust technique. We recommend further research to provide additional evidence that may inform management guidelines for clearing foreign body upper airway obstruction.
Notes from Days 2 & 3 of the London Trauma Conference
Day 2 of the LTC was really good. There were some cracking speakers who clearly had the ‘gift’ when it comes to entertaining the audience. No death by PowerPoint here (although it seems Keynote is now the presentation software of choice!). The theme of the day was prehospital care and major incidents.
The golden nuggets to take away include: (too many to list all of course)
‘Pull’ is the key to rapid extrication from cars if time critical from the Norweigan perspective. Dr Lars Wik of the Norweigen air ambulance presented their method of rapid extrication. Essentially they drag the car back on the road or away from what ever it has crashed into to control the environment and make space (360 style). They put a paramedic in the car whilst this is happening. They then make a cut in the A post near the roof, secure the rear of the car to a fire truck or fixed object with a chain and put another chain around the lower A post and steering wheel that is then winched tight. This has the effect of ‘reversing’ the crash and a few videos showed really fast access to the patient. The car seems to peel open. As they train specifically for it, there doesn’t seem to be any safety problems so far and its much quicker than their old method. I guess it doesnt matter really how you organise a rapid extrication method as long as it is trained for and everyone is on the same page.
Dr Bob Winter presented his thoughts on hangings – to date no survivor of a non-judicial hanging has had a C-spine injury, so why do we collar them? Also there seems no point in cooling them. All imaging and concern for these patients should be based on the significant soft tissue injury that can be caused around the neck.
Drownings – if the patient is totally submerged probably reasonable to search for 30mins in water that is >6 degrees or 90mins if <6 degrees. After that it becomes a body recovery (unless there is an air pocket or some exceptional circumstance). Patients that have drowned should have early ventilatory support if they show any signs of resp distress.
Drs Julian Thompson and Mark Byers reassured us on a variety of safety issues at major incidents. It seems the risk to rescuers from secondary bombs at scene is low. Very few terrorist attacks world wide, ever, have had secondary devices so rescuers should be reassured (a bit). Greatest risk to the rescuer, like always, are the silly simple things that are a risk every day, like tripping over your own feet! With reference to chemical incidents, simple PPE seems to be sufficient for the vast majority of incidents, even fairly significant chemical ones, all this mucking about in full air tight suits is probably pointless and means patients cant be treated (at all). This led to the debate of how much risk should we, as rescue staff, accept? Clearly there are no absolute answers but minimising all risk to the rescuer is often at conflict with your ability to rescue. Where the balance should lie is a matter for organisations and individuals I guess.
Sir Prof Keith Porter also gave us an update on the future of Prehospital emergency medicine as a recognised medical specialty. As those in the know, know, the specialty has been recognised by the GMC and the first draft of trainees are currently in post. More deaneries will be following suit soon to begin training but it is likely to take some time to build up large numbers of trained specialists. Importantly for those of us who already have completed our training there will be an option to sub specialise in PHEM but it will involve undertaking the FIMC exam. Great, more exams – see you there.
Day 3 – Major trauma
The focus of day 3 was that of damage control. Damage control surgery and damage control resucitation. We had indepth discussions about how to manage pelvic trauma and some of the finer points of trauma resuscitation.
Specific points raised were:
Pelvic binders are great and can replace an ex fix if the abdomen needs opening to fix a spleen for example.
You can catheterise patients with pelvic fractures (one gentle try).
Most pelvic bleeds are venous which is why surgeons who can pack a pelvis is better than a radiologist who can mainly only treat arterial bleeds.
Coagulopathy in trauma is not DIC and is probably caused by peripheral hypoperfusion.
All the standard clotting tests that we use (INR etc) are useless and take too long to do. ROTEM or TEG is much better but still not perfect.
Also, as I am sure will please many – pressure isn’t flow so dont use pressors in trauma!
Chris Hill is an emergency and prehospital care physician based in the United Kingdom