

This is a guest post from Dr Per Bredmose, anaesthetist and retrieval medicine physician in Norway, also known as Viking One
I struggle to ventilate the patient in the resus room, airway pressures are high, the bag doesn’t empty properly. In my mind I plan ahead for the next step. Through my mind goes the thought – is this the one, the one that I cannot ventilate? Statistically it is not likely to be, but I am prepared to add two-person technique, airway adjuncts like nasopharyngeal or oropharyngeal, or supraglottic devices that I use frequently in theatre. I feel confident in the use of these methods, and (in the worst case) in cricothyroidotomy. I have practiced that numerous times on our live-tissue course on anaesthetised pigs. However – before I start any of these actions.. I routinely, almost as a reflex from theatre turn the patient’s head 45 degrees to the left, and then the bag suddenly empties easily – and I can ventilate the patient.
Some people think that time with TIVA in theatre has little value for emergency medicine and advanced prehospital care. I strongly disagree. This is some of the most relevant and valuable time I have for keeping and optimising my practical skills. Bag-valve-mask (BVM) ventilation is an essential core skill for any prehospital provider. In theatre this manoeuvre is well known and frequently practiced. It is my impression that this head rotation is less used, and even maybe less well known outside theatre, and especially in the prehospital field. Therefore this is a reminder of an old technique.
When to do it: When encountering difficulties in conventional BVM ventilation, either when you cannot ventilate or when it’s just difficult to ventilate.
How to do it: Keep a firm one hand grip and gently rotate the head 45 degrees towards the side of the hand with the jaw grip. At the same time, one can try to optimise the one-hand-jaw thrust that goes along with BVM ventilation. Occasionally one needs to extend (dorsiflex) the neck a bit further to fully open the airway. The technique can also be used as a two-person technique, although this is rarely needed.
Opposition: Frequently I hear that I cannot transfer practice from theatre to the prehospital field. Well, this seems to work well in theatre, in ICU and in the field – airways are airways!!
Recently an article in European Journal of Anaesthesiology by Itagaki et al(1) with a cross over design showed an increase in tidal volume when the patients were ventilated in a head rotated position compared to neutral position with the same airway pressure. Their conclusion was as follows: Head rotation of 45° in anaesthetised apnoeic adults significantly increases the efficiency of mask ventilation compared with the neutral head position. Head rotation is an effective alternative to improve mask ventilation if airway obstruction is encountered. Therefore – this is a useful tool that one always should have in the “practical toolbox”. It is not always the solution, but occasionally it saves you (and the patient) a lot of trouble.
I haven’t used this approach and wasn’t aware of previous research showing an increase in the retroglossal (but not retropalatine) spaces in (awake) patients with head rotation(2).
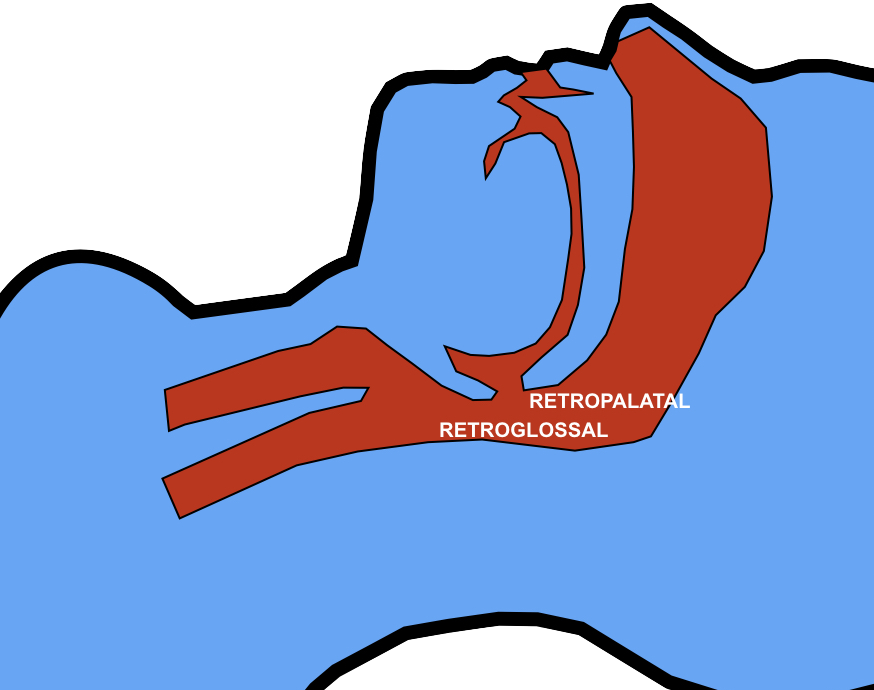
The mechanism is thought to be gravitational. It is also possible that neck rotation increases upper airway wall tension that reduces collapsibility of the lumen.
In this elegantly designed new study, a two handed BMV technique was used, similar to that advocated in my prehospital & emergency medicine environments. The rotation was always to the right, although the authors comment that they would expect the same results on the left. The increased tidal volume effect with head rotation occurred mostly in younger patients and patients with Mallampati classification I. Such patients are unlikely to be difficult to mask-ventilate, limiting the applicability of these findings to patients who are difficult to ventilate. However having one more option to employ to improve BMV efficacy (after two person technique, optimising ear-to-sternal-notch positioning, and inserting oro- and/or nasopharyngeal airways) may be useful, and the experience and perspective of my anaesthetic colleague Viking One is definitely food for thought. Obviously one should avoid this if there is potential neck injury so I won’t be trying it my trauma patients.
1. Itagaki T, Oto J, Burns SM, Jiang Y, Kacmarek RM, Mountjoy JR. The effect of head rotation on efficiency of face mask ventilation in anaesthetised apnoeic adults. Eur J Anaesthesiol. 2017 Jul;34(7):432–40.
2. Ono T, Otsuka R, Kuroda T, Honda E, Sasaki T. Effects of head and body position on two- and three-dimensional configurations of the upper airway. J Dent Res. 2000 Nov;79(11):1879–84.