
Splinted any pelvises lately? Karim Brohi’s excellent trauma.org article outlines the strengths and weaknesses of the different devices on the market. One such is the T-POD, which has now been described in a small series in which its application to patients with unstable pelvic injury was associated with improved haemodynamics and decreased symphyseal diastasis.

Here’s a video demonstrating application of the device.
Effect of a new pelvic stabilizer (T-POD1) on reduction of pelvic volume and haemodynamic stability in unstable pelvic fractures
Injury Volume 41, Issue 12, December 2010, Pages 1239-1243 (Full text)
Category Archives: Trauma
Care of severely injured patient
Massive haemorrhage guideline
The Association of Anaesthetists of Great Britain and Ireland has published guidelines on the management of massive haemorrhage. Their summary:
- Hospitals must have a major haemorrhage protocol in place and this should include clinical, laboratory and logistic responses.
- Immediate control of obvious bleeding is of paramount importance (pressure, tourniquet, haemostatic dressings).
- The major haemorrhage protocol must be mobilised immediately when a massive haemorrhage situation is declared.
- A fibrinogen < 1 g.l)1 or a prothrombin time (PT) and activated partial thromboplastin time (aPTT) of > 1.5 times normal represents established haemostatic failure and is predictive of microvascular bleeding. Early infusion of fresh frozen plasma (FFP; 15 ml.kg)1) should be used to prevent this occurring if a senior clinician anticipates a massive haemorrhage.
- Established coagulopathy will require more than 15 ml.kg)1 of FFP to correct. The most effective way to achieve fibrinogen replacement rapidly is by giving fibrinogen concentrate or cryoprecipitate if fibrinogen is unavailable.
- 1:1:1 red cell:FFP:platelet regimens, as used by the military, are reserved for the most severely traumatised patients.
- A minimum target platelet count of 75 · 109.l)1 is appropriate in this clinical situation.
- Group-specific blood can be issued without performing an antibody screen because patients will have minimal circulating antibodies. O negative blood should only be used if blood is needed immediately.
- In hospitals where the need to treat massive haemorrhage is frequent, the use of locally developed shock packs may be helpful.
- Standard venous thromboprophylaxis should be commenced as soon as possible after haemostasis has been secured as patients develop a prothrombotic state following massive haemorrhage.
Blood transfusion and the anaesthetist: management of massive haemorrhage – full document
Ketamine for HEMS intubation in Canada
Ketamine was used by clinical staff from the The Shock Trauma Air Rescue Society (STARS) in Alberta to facilitate intubation in both the pre-hospital & in-hospital setting (with a neuromuscular blocker in only three quarters of cases). Changes in vital signs were small despite the severity of illness in the study population.

A prospective review of the use of ketamine to facilitate endotracheal intubation in the helicopter emergency medical services (HEMS) setting
Emerg Med J. 2010 Oct 6. [Epub ahead of print]
Scene times & penetrating trauma
An observational cohort study of penetrating trauma patients treated by the Mobile Emergency Care Unit in Copenhagen, Denmark over a seven-and-a-half year period sought to determine the effect of on-scene time on 30-day mortality.
In this setting, in cases of penetrating trauma to the chest, or abdomen, a Mobile Emergency Care Unit (MECU) and Basic Life Support unit are dispatched simultaneously, and rendezvous at the site of the incident. The MECU is staffed with consultants in anaesthesiology, intensive care and emergency medicine, as well as a specially trained ALS provider.

The physician manning the MECU administers medication and is able to perform procedures such as intubation, thoracocentesis, pleural drainage, intravenous and intraosseous access for fluid resuscitation. Although some patients were in cardiac arrest due to penetrating torso trauma (9 patients received chest compressions, and all were dead at 30 follow up), thoracotomy was not listed as a skill provided.
Of the 467 patients registered, 442 (94.6%) were identified at the 30-day follow-up, of whom 40 (9%) were dead. A higher mortality was found among patients treated on-scene for more than 20 min (p<0.0001), although on-scene time was not a significant predictor of 30-day mortality in the multivariate analysis; OR 3.71, 95% CI 0.66 to 20.70 (p<0.14). The number of procedures was significantly correlated to a higher mortality in the multivariate analysis.
The authors conclude that on-scene time might be important in penetrating trauma, and ALS procedures should not delay transport to definite care at the hospital. However their adjusted Odds Ratio for on scene time >20 minutes as a predictor of 30 day mortality was 3.71 with very wide 95% confidence intervals (0.66 to 20.70) and there were several weaknesses and confounding factors in the study which the authors acknowledge.
The only real information this study provides appears to be on the idiosyncrasies of the Copenhagen pre-hospital care system. Looking at their list of procedures and their practice of chest compressions in cardiac arrest due to penetrating trauma, it is very hard to ascertain what, if any, advantage their physicians offer over trained paramedics. As the authors point out: “Currently, strict guidelines are not practiced. Hence, the decision to treat by a ‘scoop and run’ or a ‘stay and play’ approach is at the discretion of the physician”
On-scene time and outcome after penetrating trauma: an observational study
Emerg Med J. 2010 Oct 9. [Epub ahead of print]
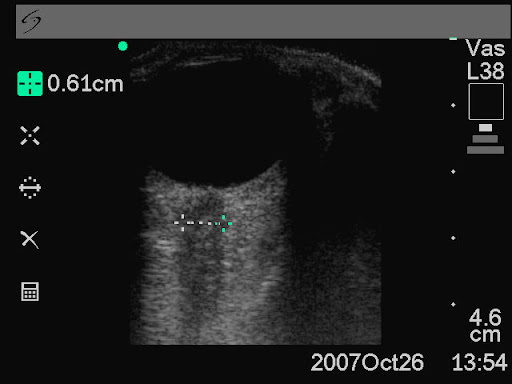
Ultrasound measurement of optic nerve sheath diameter
Here’s the abstract from a new study contributing the literature on ED assessment of raised intracranial pressure using ocular ultrasound:
Background To assess if ultrasound measurement of the optic nerve sheath diameter (ONSD) can accurately predict the presence of raised intracranial pressure (ICP) and acute pathology in patients in the emergency department.
Methods This 3-month prospective observational study used ultrasound to measure the ONSD in adult patients who required CT from the emergency department. The mean ONSD from both eyes was measured using a 7.5 MHz ultrasound probe on closed eyelids. A mean ONSD value of >0.5 cm was taken as positive. Two radiologists independently assessed CT scans from patients in the study population for signs of raised ICP and signs of acute pathology (cerebrovascular accident, subarachnoid, subdural or extradural haemorrhage and tumour). Specificity, sensitivity and k values, for interobserver variability between reporting radiologists, were generated for the study data.
Results In all, 26 patients were enrolled into the study. The ONSD measurement was 100% specific (95% CI 79% to 100%) and 86% sensitive (95% CI 42% to 99%) for raised ICP. For any acute intracranial abnormality the value of ONSD was 100% specific (95% CI 76% to 100%) and 60% sensitive (95% CI 27% to 86%). k Values were 0.91 (95% CIs 0.73 to 1) for identification of raised ICP on CT and 0.84 (95% CIs 0.62 to 1) for any acute pathology on CT, between the radiologists.
Conclusions This study shows that ultrasound measurement of ONSD is sensitive and specific for raised ICP in the emergency department. Further observational studies are needed but this emerging technique could be used to focus treatment in unstable patients.
Ultrasound measurement of optic nerve sheath diameter in patients with a clinical suspicion of raised intracranial pressure
Emerg Med J. 2010 Aug 15. [Epub ahead of print]
Pre-hospital RSI by different specialties
This aim of the study was to evaluate the tracheal intubation success rate of doctors drawn from different clinical specialities performing rapid sequence intubation (RSI) in the pre-hospital environment operating on the Warwickshire and Northamptonshire Air Ambulance. Over a 5-year period, RSI was performed in 200 cases (3.1/month).

Failure to intubate was declared if >2 successive attempts were required to achieve intubation or an ETT could not be placed correctly necessitating the use of an alternate airway. Successful intubation occurred in 194 cases, giving a failure rate of 3% (6 cases, 95% CI 0.6 to 5.3%). While no difference in failure rate was observed between emergency department (ED) staff and anaesthetists (2.73% (3/110, 95% CI 0 to 5.7%) vs 0% (0/55, 95% CI 0 to 0%); p=0.55), a significant difference was found when non-ED, non- anaesthetic staff (GP and surgical) were compared to anaesthetists (10.34% (3/29, 95% CI 0 to 21.4%) vs 0%; p=0.04). There was no significant difference associated with seniority of practitioner (p=0.65). The authors conclude that non-anaesthetic practitioners have a higher tracheal intubation failure rate during pre-hospital RSI, which may reflect a lack of training opportunities.
The small numbers of ‘failure’ rates, combined with the definition of failure in this study, make it hard to draw generalisations. Of note is that the paper lists the outcomes of the six patients who met the failed intubation definition, all of whom appear to have had their airway satisfactorily maintained by the RSI practitioner, three by eventual tracheal intubation, one by LMA, and two by surgical airway. More data are needed before whole specialties are judged on the performance of a small group of doctors.
Should non-anaesthetists perform pre-hospital rapid sequence induction? an observational study
Emerg Med J. 2010 Jul 26. [Epub ahead of print]
EM trainee RSI experience
A single centre observational study of rapid sequence intubation (RSI) was performed in a Scottish Emergency Department (ED) over four and a quarter years, followed by a postal survey of ED RSI operators.
There were 329 RSIs during the study period. RSI was performed by emergency physicians (both trained specialists and training grade, or ‘registrar’ doctors) in 288 (88%) patients. Complication rates were low and there were only two failed intubations requiring surgical airways (0.6%). ED registrars were the predominant RSI operator, with 206 patients (63%). ED consultants performed RSIs on 82 (25%) patients, anaesthetic registrars on 31 (9.4%) patients, and anaesthetic consultants on 8 (2.4%) patients. An ED consultant was present during every RSI performed and an anaesthetist was present during 72 (22%). The average number of ED registrars during this period of training was 8. This equates to each ED trainee performing approximately 26 ED RSIs (6.5 RSIs/year). On average, ED consultants performed 14 RSIs during this period (approx 3.5 RSIs/year). Of the 17 questionnaires, 12 were completed, in all of which cases the trainees were confident to perform RSI independently at the end of registrar training. Interestingly, 45 (14%) of the RSIs in the study were done in the pre-hospital environment by ED staff, two thirds of which were done by ED consultants.
Training and competency in rapid sequence intubation: the perspective from a Scottish teaching hospital emergency department
Emerg Med J. 2010 Sep 15. [Epub ahead of print]
New CPR Guidelines
The International Liaison Committee on Resuscitation has published its five-yearly update of resuscitation guidelines.
The American Heart Association Guidelines can be accessed here
The European Resuscitation Guidelines can be accessed here
2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science
Circulation. 2010;122:S639
Evidence refutes ATLS shock classification
I have always had a problem with the ATLS classification of hypovolaemic shock, and omit it from teaching as any clinical applicability and reproducibility seem to be entirely lost on me. I was therefore reassured to read that real physiological data from the extensive national trauma registry in the UK (TARN) of 107,649 adult blunt trauma patients do not strongly support this classification. A key observation we regularly make in trauma patients is the frequent presence of normo- or bradycardia in hypovolaemic patients, which is well documented in the literature.

An excellent discussion section in this paper states: ‘it is clear that the ATLS classification of shock that associates increasing blood loss with an increasing heart rate, is too simplistic. In addition, blunt injury, which forms the majority of trauma in the UK, is usually a combination of haemorrhage and tissue injury and the classification fails to consider the effect of tissue injury‘
Testing the validity of the ATLS classification of hypovolaemic shock
Resuscitation. 2010 Sep;81(9):1142-7
Burr holes by emergency physicians
Emergency physicians at Hennepin County Medical Centre (HCMC) are trained in skull trephination (drilling a burr hole) for patients with coma, anisocoria and epidural (extradural) haematoma (EDH) who have not responded to osmotic agents and hyperventilation. This may be particularly applicable in centres remote from neurosurgical centres where delays caused by interfacility transfer are associated with increased morbidity and mortality.
Dr Smith and colleagues from HCMC describe a series of five talk-and-deteriorate patients with EDH who underwent skull trephination. 3 had complete recovery without disability, and 2 others had mild to moderate disability but with good to excellent cognitive function. None had complications from the procedure other than external bleeding from the already lacerated middle meningeal artery. In 4 of 5 cases, the times were recorded. Mean time from ED presentation to trephination was 55 min, and mean time from ED to craniotomy was 173 min. The mean time saved was 118 min, or approximately 2 h.
All trephinations were done by emergency physicians, who had received training in skull trephination as part of the HCMC Emergency Medicine Residency or as part of the Comprehensive Advanced Life Support (CALS) course. Training was very brief and involved discussion of the treatment of EDH, review of a CT scan of EDH, and hands-on practice on the skull of a dead sheep, using the Galt trephinator.

An excellent point made by the authors reminds us that patients with EDH who talk-and-deteriorate (those with the traditionally described “lucid interval”) have minimal primary brain injury and frequently have no brain parenchymal injury. Thus, if the EDH is rapidly decompressed, the outcome is significantly better than for deterioration due to other aetiologies. The authors recommend in EDH that the procedure should be done within 60–90 min of onset of anisocoria. A review of other studies on the procedure would suggest that case selection is critical in defining the appropriateness of the procedure: talk-and-deteriorate, coma, anisocoria, and a delay to neurosurgical decompression.
Emergency Department Skull Trephination for Epidural Hematoma in Patients Who Are Awake But Deteriorate Rapidly
J Emerg Med. 2010 Sep;39(3):377-83