
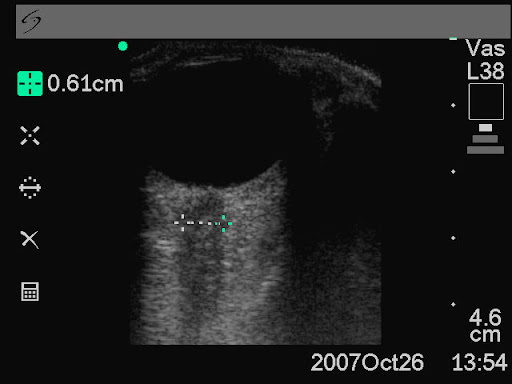
Ultrasound-guided subclavian vein cannulation has reduced complications, but there is still a high incidence of failure to cannulate the vein and of accidental arterial cannulation. Vassallo & Bennett noticed that a fast running intravenous infusion in the ipsilateral arm of a patient produced variable echogenicity (lighter echos) in the subclavian vein. They describe deliberately using this appearance to both identify the subclavian vein and differentiate it from the subclavian artery.
With the intravenous infusion running with frequent drips in the drip chamber, the ultrasound beam is placed in long axis to the subclavian vessels in the subclavicular position. The angle of the ultrasound beam is adjusted to reveal both the subclavian vein and artery. The variable echogenicity, together with compression, can then be used to identify the vein. The presence of variable echogenicity in the vessel gives continuous feedback that the ultrasound beam has not drifted onto the artery. In cases where the ultrasound beam has included both artery and vein in the same image, this method has clearly identified the intended target vessel.
Subclavian cannulation with ultrasound: a novel method
Anaesthesia, 2010;65:1041
Monthly Archives: October 2010
Scene times for rural retrieval in Scotland
The Emergency Medical Retrieval Service (EMRS) provides an aeromedical retrieval service to remote and rural communities in Scotland. They examined 300 retrievals over a five year period and showed a correlation between amount of critical care interventions required and total time on scene (defined as the total length of time between the aircraft landing and taking off from the scene, this includes access to patient, transfer to the helicopter and packaging for flight departure). Median scene time for both medical and trauma patients was 60 minutes.

The authors remind us that critical care secondary retrieval from rural healthcare facilities has many similarities to prehospital care (primary retrieval), and therefore consideration of scene times is of interest.
On-scene times and critical care interventions for an aeromedical retrieval service
Emerg Med J. 2010 Aug 19. [Epub ahead of print]
Paediatric arrest outcomes
A study of out-of-hospital paediatric arrests in Melbourne gives some useful outcome data: overall, paediatric victims of out-of-hospital cardiac arrest survived to leave hospital in 7.7% of cases, which is similar to adult survival in the same emergency system (8%). Survival was very rare (<1%) unless there was return of spontaneous circulation prior to hospital arrival. Sixteen of the 193 cases studied had trauma, but the survival in this subgroup was not specifically documented.
Epidemiology of paediatric out-of-hospital cardiac arrest in Melbourne, Australia
Resuscitation. 2010 Sep;81(9):1095-100
Ketamine for HEMS intubation in Canada
Ketamine was used by clinical staff from the The Shock Trauma Air Rescue Society (STARS) in Alberta to facilitate intubation in both the pre-hospital & in-hospital setting (with a neuromuscular blocker in only three quarters of cases). Changes in vital signs were small despite the severity of illness in the study population.

A prospective review of the use of ketamine to facilitate endotracheal intubation in the helicopter emergency medical services (HEMS) setting
Emerg Med J. 2010 Oct 6. [Epub ahead of print]
Scene times & penetrating trauma
An observational cohort study of penetrating trauma patients treated by the Mobile Emergency Care Unit in Copenhagen, Denmark over a seven-and-a-half year period sought to determine the effect of on-scene time on 30-day mortality.
In this setting, in cases of penetrating trauma to the chest, or abdomen, a Mobile Emergency Care Unit (MECU) and Basic Life Support unit are dispatched simultaneously, and rendezvous at the site of the incident. The MECU is staffed with consultants in anaesthesiology, intensive care and emergency medicine, as well as a specially trained ALS provider.

The physician manning the MECU administers medication and is able to perform procedures such as intubation, thoracocentesis, pleural drainage, intravenous and intraosseous access for fluid resuscitation. Although some patients were in cardiac arrest due to penetrating torso trauma (9 patients received chest compressions, and all were dead at 30 follow up), thoracotomy was not listed as a skill provided.
Of the 467 patients registered, 442 (94.6%) were identified at the 30-day follow-up, of whom 40 (9%) were dead. A higher mortality was found among patients treated on-scene for more than 20 min (p<0.0001), although on-scene time was not a significant predictor of 30-day mortality in the multivariate analysis; OR 3.71, 95% CI 0.66 to 20.70 (p<0.14). The number of procedures was significantly correlated to a higher mortality in the multivariate analysis.
The authors conclude that on-scene time might be important in penetrating trauma, and ALS procedures should not delay transport to definite care at the hospital. However their adjusted Odds Ratio for on scene time >20 minutes as a predictor of 30 day mortality was 3.71 with very wide 95% confidence intervals (0.66 to 20.70) and there were several weaknesses and confounding factors in the study which the authors acknowledge.
The only real information this study provides appears to be on the idiosyncrasies of the Copenhagen pre-hospital care system. Looking at their list of procedures and their practice of chest compressions in cardiac arrest due to penetrating trauma, it is very hard to ascertain what, if any, advantage their physicians offer over trained paramedics. As the authors point out: “Currently, strict guidelines are not practiced. Hence, the decision to treat by a ‘scoop and run’ or a ‘stay and play’ approach is at the discretion of the physician”
On-scene time and outcome after penetrating trauma: an observational study
Emerg Med J. 2010 Oct 9. [Epub ahead of print]
Ultrasound measurement of optic nerve sheath diameter
Here’s the abstract from a new study contributing the literature on ED assessment of raised intracranial pressure using ocular ultrasound:
Background To assess if ultrasound measurement of the optic nerve sheath diameter (ONSD) can accurately predict the presence of raised intracranial pressure (ICP) and acute pathology in patients in the emergency department.
Methods This 3-month prospective observational study used ultrasound to measure the ONSD in adult patients who required CT from the emergency department. The mean ONSD from both eyes was measured using a 7.5 MHz ultrasound probe on closed eyelids. A mean ONSD value of >0.5 cm was taken as positive. Two radiologists independently assessed CT scans from patients in the study population for signs of raised ICP and signs of acute pathology (cerebrovascular accident, subarachnoid, subdural or extradural haemorrhage and tumour). Specificity, sensitivity and k values, for interobserver variability between reporting radiologists, were generated for the study data.
Results In all, 26 patients were enrolled into the study. The ONSD measurement was 100% specific (95% CI 79% to 100%) and 86% sensitive (95% CI 42% to 99%) for raised ICP. For any acute intracranial abnormality the value of ONSD was 100% specific (95% CI 76% to 100%) and 60% sensitive (95% CI 27% to 86%). k Values were 0.91 (95% CIs 0.73 to 1) for identification of raised ICP on CT and 0.84 (95% CIs 0.62 to 1) for any acute pathology on CT, between the radiologists.
Conclusions This study shows that ultrasound measurement of ONSD is sensitive and specific for raised ICP in the emergency department. Further observational studies are needed but this emerging technique could be used to focus treatment in unstable patients.
Ultrasound measurement of optic nerve sheath diameter in patients with a clinical suspicion of raised intracranial pressure
Emerg Med J. 2010 Aug 15. [Epub ahead of print]
Cirrhotic patients on ICU
The prognosis of cirrhotic patients with multiple organ failure is not universally dismal. A retrospective French study examined predictive factors of mortality and concluded: In-hospital survival rate of intensive care unit- admitted cirrhotic patients seemed acceptable, even in patients requiring life-sustaining treatments and/or with multiple organ failure on admission. The most important risk factor for in-hospital mortality was the severity of nonhematologic organ failure, as best assessed after 3 days. A trial of unrestricted intensive care for a few days could be proposed for select critically ill cirrhotic patients.
Cirrhotic patients in the medical intensive care unit: Early prognosis and long-term survival
Crit Care Med. 2010 Nov;38(11):2108-2116
Small bowel obstruction
When assessed against CT as gold standard, ultrasound diagnosis of small bowel obstruction by emergency physicians compared favourably with abdominal radiographs.

US exams were performed using a phased array probe in the bilateral colic gutters, epigastric and suprapubic regions to assess for (1) the presence of fluid-filled, dilated bowel (defined as >25mm) proximal to normal or collapsed bowel, and (2) decreased or absent bowel peristalsis (defined as back and forth movements of spot echoes inside the fluid-filled bowel). Either finding was considered ‘positive’ for small bowel obstruction.
Bedside ultrasonography for the detection of small bowel obstruction in the emergency department
Emerg Med J. 2010 Aug 22. [Epub ahead of print]
Pre-hospital RSI by different specialties
This aim of the study was to evaluate the tracheal intubation success rate of doctors drawn from different clinical specialities performing rapid sequence intubation (RSI) in the pre-hospital environment operating on the Warwickshire and Northamptonshire Air Ambulance. Over a 5-year period, RSI was performed in 200 cases (3.1/month).

Failure to intubate was declared if >2 successive attempts were required to achieve intubation or an ETT could not be placed correctly necessitating the use of an alternate airway. Successful intubation occurred in 194 cases, giving a failure rate of 3% (6 cases, 95% CI 0.6 to 5.3%). While no difference in failure rate was observed between emergency department (ED) staff and anaesthetists (2.73% (3/110, 95% CI 0 to 5.7%) vs 0% (0/55, 95% CI 0 to 0%); p=0.55), a significant difference was found when non-ED, non- anaesthetic staff (GP and surgical) were compared to anaesthetists (10.34% (3/29, 95% CI 0 to 21.4%) vs 0%; p=0.04). There was no significant difference associated with seniority of practitioner (p=0.65). The authors conclude that non-anaesthetic practitioners have a higher tracheal intubation failure rate during pre-hospital RSI, which may reflect a lack of training opportunities.
The small numbers of ‘failure’ rates, combined with the definition of failure in this study, make it hard to draw generalisations. Of note is that the paper lists the outcomes of the six patients who met the failed intubation definition, all of whom appear to have had their airway satisfactorily maintained by the RSI practitioner, three by eventual tracheal intubation, one by LMA, and two by surgical airway. More data are needed before whole specialties are judged on the performance of a small group of doctors.
Should non-anaesthetists perform pre-hospital rapid sequence induction? an observational study
Emerg Med J. 2010 Jul 26. [Epub ahead of print]
EM trainee RSI experience
A single centre observational study of rapid sequence intubation (RSI) was performed in a Scottish Emergency Department (ED) over four and a quarter years, followed by a postal survey of ED RSI operators.
There were 329 RSIs during the study period. RSI was performed by emergency physicians (both trained specialists and training grade, or ‘registrar’ doctors) in 288 (88%) patients. Complication rates were low and there were only two failed intubations requiring surgical airways (0.6%). ED registrars were the predominant RSI operator, with 206 patients (63%). ED consultants performed RSIs on 82 (25%) patients, anaesthetic registrars on 31 (9.4%) patients, and anaesthetic consultants on 8 (2.4%) patients. An ED consultant was present during every RSI performed and an anaesthetist was present during 72 (22%). The average number of ED registrars during this period of training was 8. This equates to each ED trainee performing approximately 26 ED RSIs (6.5 RSIs/year). On average, ED consultants performed 14 RSIs during this period (approx 3.5 RSIs/year). Of the 17 questionnaires, 12 were completed, in all of which cases the trainees were confident to perform RSI independently at the end of registrar training. Interestingly, 45 (14%) of the RSIs in the study were done in the pre-hospital environment by ED staff, two thirds of which were done by ED consultants.
Training and competency in rapid sequence intubation: the perspective from a Scottish teaching hospital emergency department
Emerg Med J. 2010 Sep 15. [Epub ahead of print]