I was taught a useful principle by a paediatric anaesthetist 10 years ago which has proven true in my experience and has contributed to keeping me calm when intubating sick kids. Unlike adults, in whom difficulty in intubation can often be unexpected, the vast majority of normal looking children are easy to intubate, and the ones who are difficult usually have obvious indicators such as dysmorphism.
This appears to be supported by recent evidence: in a large retrospective series of 11.219 anaesthesia patients, the overall incidence of difficult laryngoscopy [Cormack and Lehane (CML) grade III and IV] was only 1.35%, although was much higher in infants less than one year compared with older children. This low percentage is in the same ball park as two other paediatric studies. Besides younger age, their database suggested underweight, ASA III and IV physical status and, if obtainable, Mallampati III and IV findings as predictors for difficult laryngoscopy. The authors point out:
“…the oromaxillofacial surgery department with a high proportion of cleft palate interventions and pediatric cardiac surgery contributed substantially to the total number of difficult laryngoscopies. In patients undergoing pediatric cardiac surgery, a possible explanation for the higher incidence of CML III/IV findings might be that some congenital heart defects are associated with chromosomal anomalies like microdeletion 22q11.2 syndrome. This syndrome is also associated with extracardiac anomalies like cranio-facial dysmorphism“
Take home message: As a very rough rule of thumb to illustrate the difference between the ease/difficulty of laryngoscopy between adults and kids, I think it’s fair to say grade III or IV views occur in about 10% of adults but only about 1% of children.
Incidence and predictors of difficult laryngoscopy in 11.219 pediatric anesthesia procedures Paediatr Anaesth. 2012 Aug;22(8):729-36
[EXPAND Click for abstract]
OBJECTIVE: Difficult laryngoscopy in pediatric patients undergoing anesthesia.
AIM: This retrospective analysis was conducted to investigate incidence and predictors of difficult laryngoscopy in a large cohort of pediatric patients receiving general anesthesia with endotracheal intubation.
BACKGROUND: Young age and craniofacial dysmorphy are predictors for the difficult pediatric airway and difficult laryngoscopy. For difficult laryngoscopy, other general predictors are not yet described.
METHODS: Retrospectively, from a 5-year period, data from 11.219 general anesthesia procedures in pediatric patients with endotracheal intubation using age-adapted Macintosh blades in a single center (university hospital) were analyzed statistically.
RESULTS: The overall incidence of difficult laryngoscopy [Cormack and Lehane (CML) grade III and IV] was 1.35%. In patients younger than 1 year, the incidence of CML III or IV was significantly higher than in the older patients (4.7% vs 0.7%). ASA Physical Status III and IV, a higher Mallampati Score (III and IV) and a low BMI were all associated (P < 0.05) with difficult laryngoscopy. Patients undergoing oromaxillofacial surgery and cardiac surgery showed a significantly higher rate of CML III/IV findings.
CONCLUSION: The general incidence of difficult laryngoscopy in pediatric anesthesia is lower than in adults. Our results show that the risk of difficult laryngoscopy is much higher in patients below 1 year of age, in underweight patients and in ASA III and IV patients. The underlying disease might also contribute to the risk. If the Mallampati score could be obtained, prediction of difficult laryngoscopy seems to be reliable. Our data support the existing recommendations for a specialized anesthesiological team to provide safe anesthesia for infants and neonates.
Want to access the femoral vein? Externally rotate the leg at the hip and things might be a bit easier. This study was done in adult patients, with the knee straight and no abduction applied. External rotation is also helpful in kids, with abduction up to sixty degrees.
Objective: To determine if external rotation of the leg increases the size and accessibility of the femoral vein compared with a neutral position.
Methods: One hundred patients presenting to a tertiary teaching hospital were prospectively recruited. The right common femoral vein of each subject was scanned with a linear probe (5–10 MHz) inferior to the inguinal ligament, with the leg in a neutral position and then in the externally rotated position. The transverse diameter of the femoral vein, the accessible diameter of the vein (lying medial to the femoral artery) and the depth of the vein were measured.
Results: The mean diameter of the femoral vein in the externally rotated leg was greater than with the leg in the neutral position (15.4 mm vs 13.8 mm); the mean difference was 1.6 mm (95% CI 1.3–1.9). The mean accessible diameter of the femoral vein was larger with the leg externally rotated (13.8 mm vs 11.7 mm, mean difference 2.1 mm, 95% CI 1.8–2.5). The depth from the skin to the femoral vein was less with the leg in external rotation (20.9 mm vs 22.6 mm, mean difference 1.7 mm, 95% CI 1.2–2.2). The mean diameter and depth were greater in patients with overweight or obese body mass index (BMI) measurements in both leg positions. The increase in femoral vein diameter and accessibility with external rotation was observed in all BMI groups.
Conclusion: The total and accessible femoral vein diameter is increased and the surface depth of the vein is decreased by placing the leg in external rotation compared with the neutral position.
Ever waste time trying to shake some ultrasound gel out the bottle, like a resistant blob of ketchup?
Sydney emergency medicine registrar Dr Steve Skinner demonstrates how to solve this. With physics.
This really does work, and has saved me a lot of time already. I now do a somewhat less ballistic version than the one demonstrated, so that patients don’t think I’m mad.
This video is for entertainment purposes only. We accept no responsibility for injuries sustained as a result of unaccustomed shoulder activity or inadvertently launched plastic projectiles.
During a Krav Maga self defence drill a middle aged martial arts enthusiast cleverly blocked a full contact punch with his nose. Following a suggestion to pause training to control the bleeding, he noticed some lateral nasal displacement which was easily manually reduced with an audible click. He was able to resume training with a piece of toilet paper stuffed up the bleeding nostril, and no ill effects were noticed on subsequent training nights that week.
The day after injury he demonstrated a characteristic bruising pattern:
As he was working an aeromedical retrieval shift, he was able to use the Retrieval Service Sonosite M-Turbo ultrasound machine to identify the cortical disruption from his nasal bone fracture.
Ultrasound compares favourably with both plain radiography(1) and computed tomography(2) in the diagnosis of nasal bone fractures.
Personal access to sonography and full board certification in emergency medicine help to decrease health care costs and emergency department load when individuals sustain fractures that do not require operative management(3).
Drs Wyatt and Haugh describe a modified resuscitative thoracotomy technique which provided surgically facilitated pericardial drainage. A patient with a ruptured pseudoaneurysm of the right ventricular outflow tract presented in shock and arrested in the ED. She had had a prior history of idiopathic ventricular tachycardia and had undergone cardiac ablation of the posteroseptal wall of the right ventricular outflow tract. Sonographically identified tamponade was treated with pericardiocentesis which failed due to clotted blood, so a left lateral thoracotomy was performed by the emergency physician. Rather than fully expose the heart for repair in the ED, they elected to just make a 2cm incision in the pericardium which allowed drainage of blood and restoration of circulation. This was combined with blood product transfusion to buy time for the arrival of a cardiothoracic surgeon and transfer to the operating room.
Useful learning points from this paper are:
Ablation procedures are becoming more common
Serious complications such as atrioesophageal fistula, pseudoaneurysm, pericardial effusion, and cardiac tamponade occur approximately 3% of the time
When tamponade is suspected or confirmed ask patient about recent cardiac procedures such as catheterisations, surgery, and ablation procedures
Radiofrequency ablation procedures are often performed on the right side of the heart in areas that may be relatively inaccessible from a left-sided lateral thoracotomy approach.
Modified Emergency Department Thoracotomy for Postablation Cardiac Tamponade Ann Emerg Med. 2012 Apr;59(4):265-7
[EXPAND Click for abstract]
Cardiac dysrhythmias are a common problem in the United States. Radiofrequency ablation is being used more frequently as a treatment for these diagnoses. Although rare, serious complications such as cardiac tamponade have been reported as a result of ablation procedures. Traditionally, emergency department (ED) thoracotomy has been reserved for cases of traumatic arrest only. We report a case of a successful modified ED thoracotomy in a patient with postablation cardiac tamponade and subsequent obstructive shock who failed intravenous fluid resuscitation, pressor administration, and multiple attempts at pericardiocentesis. In this case, a modified approach was used to incise the pericardium. Although this was associated with large blood loss, we believed that using the traditional method of completely removing the pericardium would have resulted in uncontrolled hemorrhage. Instead, our method led to successful resuscitation of the patient until definitive care was available. A smaller pericardial incision than is traditionally used during ED thoracotomy deserves further consideration and research to determine whether and when it may be most useful as a temporizing treatment of cardiac tamponade when other methods have failed.
In resuscitation situations, the securing of vascular catheters is an important but sometimes cumbersome process, particular when sutures are required for central lines or arterial lines.
Medical grade ‘superglue’ (cyanoacrylate) can be used and this has been described in the anaesthetic literature before(1). Now, further in vitro work shows the glue does not weaken the intravenous catheter and is not associated with bacterial colonisation(2).
I think this is perfect for resuscitation lines. Just last night I used this technique to secure a femoral arterial line during a cardiac arrest resuscitation. It was great not to have to faff around with sharp suture needles during CPR and the line felt very secure after just a few seconds.
A burns patient whose tracheal tube was accidentally dislodged and ended up placed in the oesophagus on day 2 of his ICU stay continued to spontaneously ventilate and maintain saturations on a midazolam infusion. The oesophageal tube was left in during laryngoscopy (after propofol but no muscle relaxant due to anticipated difficult airway) which revealed a cormack-lehane grade 3 view. The operator’s hand which was holding a bougie rested on the oesophageal tube, which displaced it backwards. This resulted in backwards displacement of the larynx and improved the glottic view to 2b, facilitating intubation.
The discovery of this ‘backwards internal laryngeal pressure’ manoeuvre led the authors to make the recommendation that during difficult intubation an inadvertently placed oesophageal tube should be left in place to allow a BILP manouevre, but removed if it impedes the passage of the tracheal tube.
I love anything that might improve success rates of critical procedures and this one could conceivably come in handy. I can just see Minh Le Cong inventing a transoesophageal posterior laryngal retractor for under 50 bucks… The use of “Internal Laryngeal Pressure” to improve the laryngeal view following inadvertent oesophageal intubation in a patient with difficult airway Anaesth Intensive Care. 2012 Jul;40(4):736-7
A case is reported in Prehospital Emergency Care1 in which an agitated patient (due to mania and alcohol intoxication) received 5 mg/kg (500 mg) of ketamine intramuscularly by an EMS crew which dissociated him within a few minutes. He subsequently developed episodes of laryngospasm in the emergency department which were unrelieved by head tilt, chin lift and simple airway adjuncts but responded to bag-mask ventilation (BMV). The patient was intubated because the laryngospasm recurred, although it had again responded to BMV.
The authors make the point that because of the response of laryngospasm to simple manoeuvres, and because in the prehospital environment a patient will not be left without an EMS provider present, ‘restricting ketamine to EMS units capable of rapid-sequence intubation therefore seems unnecessary.‘
This is one for EMS directors to consider seriously. Personally, I think practicing prehospital care without access to ketamine is like having a hand tied behind my back. Ketamine opens up a world of possibilities in controlling combative patients, optimising scene safety, providing sedation for painful procedures including extrication, and enabling severe pain to be controlled definitively.
I’ve been using ketamine regularly for prehospital analgesia and emergency department procedural sedation in both adults and kids for more than a decade. I’ve seen significant laryngospasm 5 times (twice in kids). On one of those occasions, a 3 year old child desaturated to around 50% twice during two episodes of laryngospasm. We weren’t slow to pick it up – that was just her showing us how quickly kids can desaturate which continued while we went through a stepwise approach until BMV resolved it. It was however an eye opener for the registrar (senior resident) assisting me, who became extremely respectful of ketamine after that. Our ED sedation policy (that I wrote) required that suxamethonium was ready and available and that an appropriate dose had been calculated before anyone got ketamine. Paralysis may extremely rarely be required, but when it’s needed you need to be ready.
The best monitor for laryngospasm – noninvasive capnography
Laryngospasm is rare but most regular prescribers of ketamine will have seen it; the literature says it occurs in about 1-2% of sedations, although anecdotally I think it’s a bit less frequent. Importantly for those weighing the risks of allowing non-RSI competent prescribers, the requirement for intubation is exceptionally rare (2 of 11,589 reported cases in one review). Anyone interested should read this excellent review of ketamine-related adverse effects provided by Chris Nickson at Life in The Fast Lane. Chris reminds us of the Larson manouevre, which is digital pressure in the notch behind and below the ear, described by Larson2 as follows:
The technique involves placing the middle finger of each hand in what I term the laryngospasm notch. This notch is behind the lobule of the pinna of each ear. It is bounded anteriorly by the ascending ramus of the mandible adjacent to the condyle, posteriorly by the mastoid process of the temporal bone, and cephalad by the base of the skull. The therapist presses very firmly inward toward the base of the skull with both fingers, while at the same time lifting the mandible at a right angle to the plane of the body (i.e., forward displacement of the mandible or “jaw thrust”). Properly performed, it will convert laryngospasm within one or two breaths to laryngeal stridor and in another few breaths to unobstructed respirations.
I use this point most often to provide painful stimuli when assessing GCS in a patient, particular those I think may be feigning unconsciousness (I’ve done this for a number of years since learning how painful it can be when I was shown it by a jujitsu instructor). Dr Larson says he was taught the technique by Dr Guadagni, so perhaps we should be calling it the ‘Guadagni manouevre’. The lack of published evidence has led to some appropriate skepticism3, but as it can be combined with a jaw thrust it needn’t delay more aggressive interventions should they become necessary, it may work, and it’s likely to be harmless.
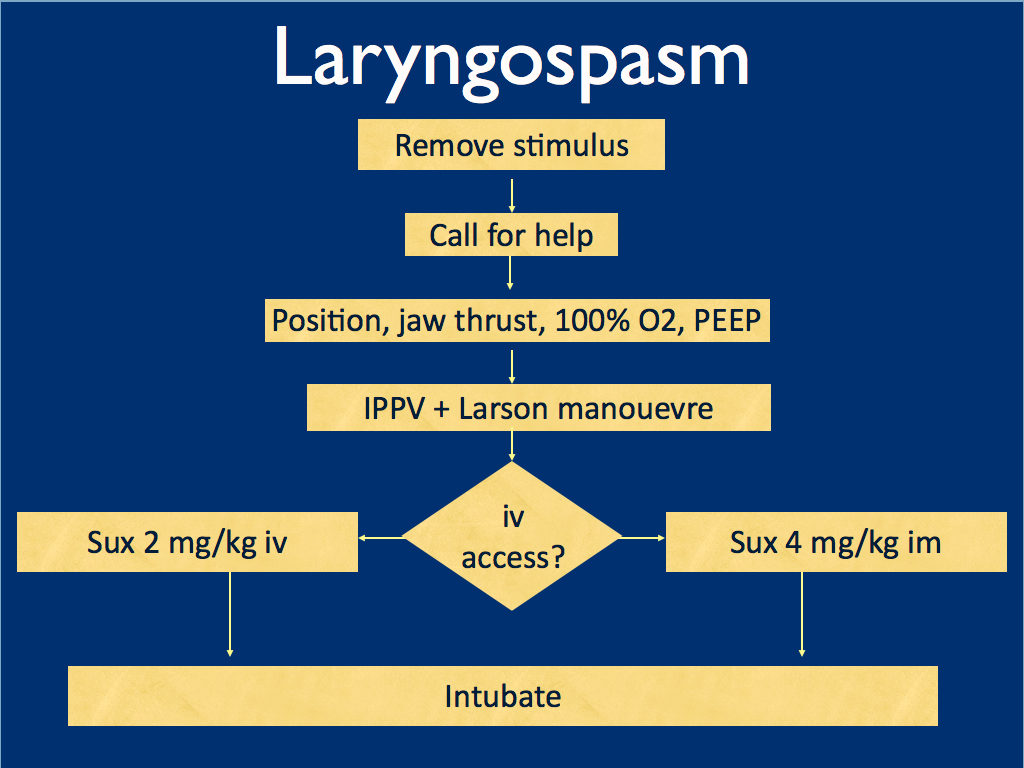
I presented the following suggested algorithm for management of laryngospasm during ketamine procedural sedation at a regional emergency medicine ‘Fellows Forum’ meeting in November 2007 in the UK. Since many paediatric procedural sedations were done using intramuscular (im) ketamine, it gives guidance based on whether or not vascular access has been obtained:
Some things I considered were:
Neuromuscular blockade (NMB) isn’t always necessary – laryngospasm may be managed with other sedatives such as propofol. However, titrating further sedatives in a desaturating child in my view is inferior to definitive airway management and laryngeal relaxation with suxamethonium and a tube.
Laryngospasm may be managed with much smaller doses of suxamethonium than are required for intubation – as little as 0.1 mg/kg may be effective. However, I think once we go down the NMB route we’re committed to intubation and therefore we should use a dose guaranteed to be effective in achieving intubating conditions.
In the child without vascular access, I considered intraosseous and intralingual sux. However, intramuscular suxamethonium is likely to have a relaxant effect on the laryngeal muscles within 30-45 seconds, which has to be compared with time taken to insert and confirm intraosseous needle placement. I do not think the traditionally recommended intralingual injection has any role to play in modern airway management.
At the time I wrote this most paediatric resuscitation bays in my area in the United Kingdom had breathing circuits capable of delivering PEEP – usually the Ayr’s T-Piece (specifically the Mapleson F system), which is why PEEP was included early in in the algorithm prior to BMV.
I have since modified it for two reasons: firstly, we might as well do the Larson manoeuvre during the jaw thrust; secondly, many Australasian and US EDs will only be able to deliver PEEP with a PEEP valve attached to a BVM, so PEEP has been moved to the BVM stage.
I would love to hear what people are doing in their prehospital and inhospital practice. Should ketamine only be administered by providers who can offer RSI? Do you have a laryngospasm protocol? If so, I’d love to see it. If not, feel free to use or adapt my unvalidated one at your own risk.
ABSTRACT An advanced life support emergency medical services (EMS) unit was dispatched with law enforcement to a report of a male patient with a possible overdose and psychiatric emergency. Police restrained the patient and cleared EMS into the scene. The patient was identified as having excited delirium, and ketamine was administered intramuscularly. Sedation was achieved and the patient was transported to the closest hospital. While in the emergency department, the patient developed laryngospasm and hypoxia. The airway obstruction was overcome with bag–valve–mask ventilation. Several minutes later, a second episode of laryngospasm occurred, which again responded to positive-pressure ventilation. At this point the airway was secured with an endotracheal tube. The patient was uneventfully extubated several hours later. This is the first report of laryngospam and hypoxia associated with prehospital administration of intramuscular ketamine to a patient with excited delirium.
This appears to be a useful option when iv access is difficult and the patient is relatively stable.
The protocol specified nebulisation of 2 mg of naloxone with 3 mL of normal saline as empiric treatment for suspected opioid overdose or undifferentiated depressed respirations as long as the patient had some spontaneous respiratory effort, no apnoea, and no severe cardiorespiratory compromise.
BACKGROUND: Emergency medical services (EMS) traditionally administer naloxone using a needle. Needleless naloxone may be easier when intravenous (IV) access is difficult and may decrease occupational blood-borne exposure in this high-risk population. Several studies have examined intranasal naloxone, but nebulized naloxone as an alternative needleless route has not been examined in the prehospital setting.
OBJECTIVE: We sought to determine whether nebulized naloxone can be used safely and effectively by prehospital providers for patients with suspected opioid overdose.
METHODS: We performed a retrospective analysis of all consecutive cases administered nebulized naloxone from January 1 to June 30, 2010, by the Chicago Fire Department. All clinical data were entered in real time into a structured EMS database and data abstraction was performed in a systematic manner. Included were cases of suspected opioid overdose, altered mental status, and respiratory depression; excluded were cases where nebulized naloxone was given for opioid-triggered asthma and cases with incomplete outcome data. The primary outcome was patient response to nebulized naloxone. Secondary outcomes included need for rescue naloxone (IV or intramuscular), need for assisted ventilation, and adverse antidote events. Kappa interrater reliability was calculated and study data were analyzed using descriptive statistics.
RESULTS: Out of 129 cases, 105 met the inclusion criteria. Of these, 23 (22%) had complete response, 62 (59%) had partial response, and 20 (19%) had no response. Eleven cases (10%) received rescue naloxone, no case required assisted ventilation, and no adverse events occurred. The kappa score was 0.993.
CONCLUSION: Nebulized naloxone is a safe and effective needleless alternative for prehospital treatment of suspected opioid overdose in patients with spontaneous respirations.
I had the honour of attending trauma rounds with leading South African trauma surgeons today at Groote Schuur Hospital in Cape Town. This was the first day of an intense week-long trauma education tour that I have organised for myself and three of my Sydney HEMS colleagues.
A technique for haemorrhage control in penetrating trauma is to place a Foley catheter (FC) in the wound and inflate the balloon to try to achieve compression of bleeding vascular structures. This has been life-saving in many cases and buys time to get the patient to a trauma or vascular surgeon or in some cases an interventional radiologist. Catheter is knotted (black arrow) to occlude lumen. The wound is sutured around the catheter (white arrow).
First described by Gilroy and colleagues from Baragwanath Hospital in Johannesburg1, another, larger case series was subsequently reported by Cape Town’s Navsaria2, the Professor who conducted today’s trauma round I attended. In his paper he describes:
An 18- or 20-G FC was introduced into the bleeding neck wound. An attempt was made to follow the wound tract. The balloon was inflated with 5 ml of water or until resistance was felt. The FC was either clamped or knotted on itself to prevent bleeding through the lumen. The neck wound was sutured in two layers around the catheter. Continued bleeding around the catheter was an indication to proceed to surgery.
There were no deaths attributable to the use of FC balloon tamponade.
Prof. Navsaria describes the following algorithm for the subsequent investigation and management of these patients:
I’ve been teaching this technique as an option in penetrating trauma for a few years but have never actually done it for real. Nice to finally see examples of its successful implementation by people who do this all the time. I’ve seen four patients with Foleys sticking out of their necks in the first 24 hours of being here.
1. Control of life-threatening haemorrhage from the neck: a new indication for balloon tamponade. Injury. 1992;23(8):557-9
[EXPAND Click to read abstract]
We report the use of a Foley catheter, placed through the wound, to provide balloon tamponade of major bleeding from the neck and supraclavicular fossae. In 10 consecutive explorations for exsanguinating injury in these regions balloon tamponade was used eight times, and was judged to be fully effective in four patients, partly effective in one, and ineffective in three patients.
[/EXPAND]
2. Foley catheter balloon tamponade for life-threatening hemorrhage in penetrating neck trauma World J Surg. 2006 Jul;30(7):1265-8
[EXPAND Click to read abstract]
BACKGROUND: Foley catheter (FC) balloon tamponade is a well-recognized technique employed to arrest hemorrhage from penetrating wounds. The aim of this study was to review our experience with this technique in penetrating neck wounds and to propose a management algorithm for patients with successful FC tamponade.
METHODS: A retrospective chart review (July 2004-June 2005 inclusive) was performed of patients identified from a prospectively collected penetrating neck injury computer database in whom FC balloon tamponade was used. The units’ policy for penetrating neck injuries is one of selective nonoperative management. All patients with successful FC tamponade underwent angiography. A venous injury was diagnosed if angiography was normal. Ancillary tests were performed as indicated. Removal of the FC was performed in the OR.
RESULTS: During the study period, 220 patients with penetrating neck injuries were admitted to our unit. Foley catheter balloon tamponade was used in 18 patients and was successful in 17 patients. Angiography was positive in 3 patients, all of whom underwent surgery. The FC was successfully removed in 13 patients at a mean of 72 (range 48-96) hours. One patient bled after removal of the catheter, mandating emergency surgery.
CONCLUSION: Foley catheter balloon tamponade remains a useful adjunct in the management of selective patients with penetrating, bleeding neck wounds.

 I was taught a useful principle by a paediatric anaesthetist 10 years ago which has proven true in my experience and has contributed to keeping me calm when intubating sick kids. Unlike adults, in whom difficulty in intubation can often be unexpected, the vast majority of normal looking children are easy to intubate, and the ones who are difficult usually have obvious indicators such as dysmorphism.
I was taught a useful principle by a paediatric anaesthetist 10 years ago which has proven true in my experience and has contributed to keeping me calm when intubating sick kids. Unlike adults, in whom difficulty in intubation can often be unexpected, the vast majority of normal looking children are easy to intubate, and the ones who are difficult usually have obvious indicators such as dysmorphism.