One of my nursing colleagues was telling a story the other day about one of the first resuscitations we did together in the ED several years ago. It demonstrates the principle of establishing control of a sub-optimally coordinated team by using some form of attention grabber. She kindly agreed to write down her recollection for me to share here:
I have finally found 2 minutes to sit down and write you the story I was telling you about the other week…. We were in the middle of a resus in the ED, it was chaotic, loud and messy.
I remember you calling out in a commanding voice for everyone to stop (can’t recall what you actually said) but when we all looked up and fell silent you lifted up one leg, let a rather loud large fart out and then very calmly proceeded to take control of the situation. Everyone was so stunned, and slightly amused that the whole situation just settled right down and we all cracked on with the resus in a much more organised fashion.
I don’t know if you know I own a first aid training company. I tell this story when I am teaching. I explain to people that an emergency situation can be chaotic and stressful and someone has to take control. Sometimes you need to take a second to get a grip of yourself and others before you can be of any help to the person in need.
By telling your story it makes people realise you can stop for a second to gather yourself, take stock of what is needed then crack on. Sometimes it takes extreme measures such as dropping a fart to get people to get back on track.
You have given me many stories over the years but the fart one has got the most traction so far.
See you at work
I accept that some people may find this offensive or consider it inappropriate or unprofessional. Please consider:
All mammals produce flatus.
Holding on to flatus can be uncomfortable and can distract a resuscitation team leader, potentially adversely affecting outcome.
The performance had its desired effect, helping the resuscitation.
The patient was intubated and therefore not at olfactory risk
Occasionally we step out of the resuscitation room feeling like a case should have gone better, but it can be hard to put our finger on just where it went wrong. In my last post I discussed the STEPS approach to analysing resuscitation cases: Self, Team, Environment, Patient and System.
Occasionally you can get a case where the STEPS seem to be aligned but things still feel bad. In which the outcome was unsatisfactory because the plan was wrong, or the team wasn’t able to execute the plan. Consider the following case.
1. A patient with a past history of DVT no longer on anticoagulants presents with chest pain and syncope.
She is severely hypotensive with a raised jugular venous pressure and a clear chest x-ray. A working diagnosis of pulmomary embolism is made.
Discussions ensue regarding empirical fibrinolysis and a respiratory physician is consulted, who over the phone cautions against treating without a CT pulmonary angiogram.
The patient is given heparin and transferred to the CT scanner where she arrests. Intravenous rtPA is given during CPR but no return of spontaneous circulation is achieved and she is pronounced dead after 30 minutes of resuscitation.
On this occasion the team worked efficiently and communicated well under clear leadership. Everyone knew the plan and shared the mental model. The environment was well controlled and the patient had been swiftly moved to CT within 20 minutes of arrival. Thanks to simulation training the well rehearsed cardiac arrest resuscitation was conducted with precision and the team was able to rapidly access the thrombolytic and knew the correct dose.
By a quick STEPS analysis, this case appears to have gone as well as could be expected. Perhaps there is nothing to learn. Some you win, some you lose, no?
No. Autopsy revealed type A aortic dissection with pericardial tamponade.
The management may have been efficient but it failed to be effective. In other words, things were done right, but the right things weren’t done; they did the wrong things right.
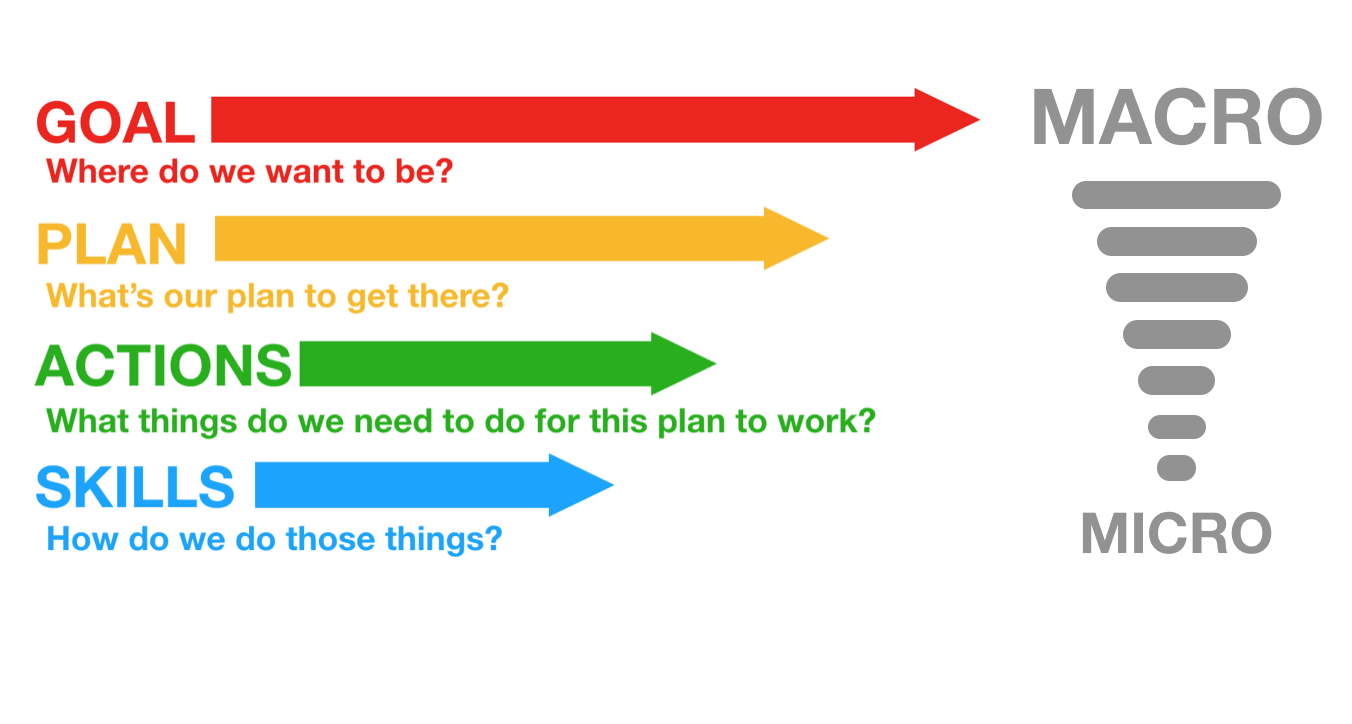
This might be an example where STEPS is inadequate, and instead we should evaluate the clinical trajectory. The cognitive bias that led to a lack of consideration of alternative diagnoses might be classifiable under ‘self’ or ‘team’ but I find it more helpful to consider it under a failure of strategy. What is strategy? Strategy in my mind is another word for plan. The plan is based on a particular resuscitation goal, and will consist of the procedures & skills required to action the plan. We can thus break down an attempted clinical trajectory into:
Goal (what are we trying to achieve) Strategy, or Plan (what’s our plan to get there?) Tactics, or Actions (what procedures will be required to execute the plan) And, at more granular level: If we’re failing at the procedural level, the components of procedures, namely Skills & Microskills. So, as we zoom in from macro to micro in setting the clinical trajectory, we can look at Goals, Plan, Actions, and Skills: In the above case it appears the following was applied, in terms of Goal-Plan-Actions-Skills:
G – resuscitate hypotensive patient P – give fibrinolysis for likely PE A – consult respiratory physician, get CTPA S – request scan, give heparin, transport to CT
The goal was appropriate, but the plan was ineffective.
The following approach would have been more effective.
G – resuscitate hypotensive patient P – identify cause of undifferentiated hypotension and initiate treatment in the resus room A – thorough bedside assessment in patient too sick to move: history, physical, CXR, ECG, labs, POCUS S – Basic cardiac ultrasound
By planning to identify and treat the cause of hypotension in the resus room, the more appropriate investigation would have been selected (cardiac ultrasound) and the correct diagnosis is much more likely to have been made.
Let’s look at some other cases:
2. An 88-year-old male presents by ambulance to the ED with dizziness. He is hypotensive, pyrexial, hypoxic and confused.
His chest x-ray shows likely bronchopneumonia. He has appropriate initial resuscitation and ICU is consulted. Soon he is intubated and on high dose vasoactive medication with escalating doses despite ongoing hypotension, anuria, and a lactate of 11 mmol/l, increased from 8 on arrival.
As he is being wheeled off down the corridor towards ICU his distraught and frail wife arrives. She is taken to the quiet room where she explains that her husband would never want to be ‘on a life support machine’ and asks ‘can’t you just keep him comfortable’?
G – the goal – to provide maximally aggressive resuscitation – was not in keeping with the patient’s wishes. If the goal had been to provide care in accordance with his wishes, the plan could have included attempts to ascertain these sooner while providing initial treatment. Upon gaining sufficient information, a new goal can be established: maximising the patient’s comfort and dignity.
3. An obese 30-year-old female presents with syncope. At triage she is pale, tachycardic & hypotensive. Clinical and sonographic assessment, including free intraperitoneal fluid and a positive urine HCG, is suggestive of ruptured ectopic pregnancy.
The gynaecologist and anaesthetist ask the ED team to bring the patient straight to the operating room. The ED team spends 20 minutes struggling to obtain intravenous access, eventually placing a 22G intravenous catheter in the patient’s hand and a humeral intraosseous needle.
Her shock is considerably worse on arrival in theatre, despite attempts to transfuse O negative blood en route.
Goal – get her safely to the operating room Plan – vascular access, cross match blood, start haemostatic resuscitation, go to OR as soon as possible Actions – peripheral and/or intraosseous cannulation attempts Skills – vascular access skills
Here the failure was at the actions and skills level. Better vascular access could have been attained using ultrasound guided peripheral cannulation, or central vascular access, or earlier intraosseous insertion.
4. A 120kg 32-year-old male with a history of deliberate self harm presents on the night shift with coma due to mixed benzodiazepine and venlafaxine overdose.
The decision is made to intubate for airway protection. After rapid sequence induction direct laryngoscopy is attempted by the emergency registrar who obtains a grade 4 view. Cricoid pressure is removed resulting in a grade 3 view.
The registrar asks for a bougie which she passes and then railroads the tracheal tube over it. The cuff is inflated, capnography is connected, and the self-inflating bag is connected and squeezed while the chest is auscultated.
The abdomen distends, the capnograph remains flat, and gastric contents are seen to pass upward through the tube into the self-inflating bag. The tube is immediately removed and bag-mask ventilation is attempted. The oxygen saturation is now 78% and the airway is soiled. The airway is suctioned and repeat attempts to bag-mask ventilate fail. A successful cricothyroidotomy is performed and the patient subsequent has full neurological recovery.
Goal – Provide supportive care and minimise complications from overdose Plan – Airway protection and admit to ICU for monitoring Actions – Rapid sequence intubation, ICU referral Skills – Pre-, peri- and post-intubation oxygenation techniques; patient positioning; rapid sequence induction of anaesthesia; direct laryngoscopy; bougie handling techniques; external laryngeal manipulation
In this case the patient was not placed in the ramped position and no nasal cannulae were applied for apnoeic oxygenation. A tube was railroaded over an oesophageal bougie, which arguably should not occur if ‘hold up’ is sought when the bougie is placed.
Although the goal, plan and actions were appropriate, the team did not demonstrate adequate skill in this procedure. Likely due to a failure of training, standardised procedures, and checklists (or their application), this could also be identified as a ‘system’ problem in STEPS. It is also possible that the intubator forgot her training under stress – a problem classifiable under ‘self’. Alternatively other members of the team may have had knowledge but didn’t speak up or cross-check their colleague, which would be a ‘team’ issue.
Limitations of this approach This sort of analysis is retrospective and subjective and at risk of hindsight bias (e.g. distortion due to projection, denial, or selective recall). However, these limitations do not negate the value of the learning exercise, particularly if we are aware of them and strive to minimise their impact (e.g. write down the details of a cases as soon as possible afterward). It at least provides a structure for individuals and teams to begin the conversation about where and how things may have been suboptimal.
Goals may be multiple and may change according to incoming information, and for each goal there may be several viable alternative plans. STEPS and GPAS may overlap, eg. team failures may result in inappropriate goals and strategies, or in failed procedures.
Summary These models may prove helpful as a means of dissecting a case in a structured way. Put simply, STEPS offers a structure for identifying efficiency improvements (“doing things right”) and GPAS can help us assess effectiveness (“doing the right things”).
Another way of looking at it is that STEPS provides the components of a resus at any point in time, and GPAS defines the trajectory: where the resus is going and how to get there.
I use this structure to analyse cases in my own clinical practice and in my teaching. I would be interested to hear from others’ experience. Do you find this approach useful in identifying areas for improvement in those cases that you feel should have gone better?
Thanks to Chris Nickson for his comments and improvements to this post
A resuscitationist agonises. These words, expressed by Scott Weingart during a podcast we did together, ring true to all of us who strive to improve our practice. Driven by the passionate conviction that we should never lose a salvageable patient through imperfect care, we relive cases and re-run them through our mental simulators to identify areas for improvement.
In the search for actionable items though, we occasionally exit this process empty-handed. Something about a case felt wrong although ostensibly all the clinical interventions may have been appropriate. It is in these cases that it can be helpful to have a structure to aid analysis.
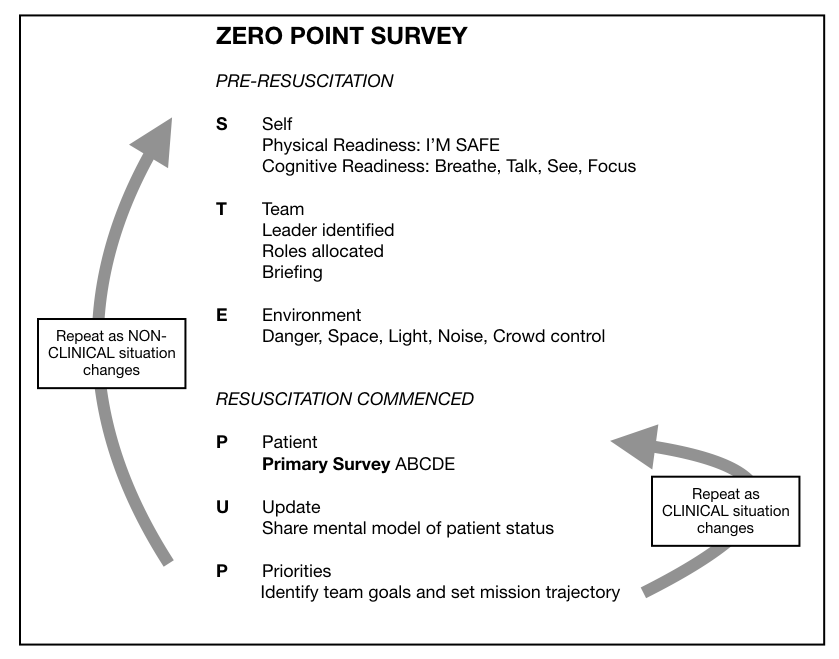
I, along with an international, interdisciplinary faculty of resuscitationists, have previously proposed an easily remembered system for optimising the clinical and non-technical components of resuscitation immediately before and during a patient encounter, dubbed the ‘Zero Point Survey’ (ZPS)(1), so called because first contact with a patient is rarely ‘Time Zero’ for a prehospital mission or hospital resuscitation case; there is invariably time for preparation of oneself, one’s team, and the environment (including equipment) prior to the primary survey and commencement of resuscitation. Following the assessment and management of STEP (self, team, environment & patient), the team should be regularly Updated on patient status and informed of the Priorities.
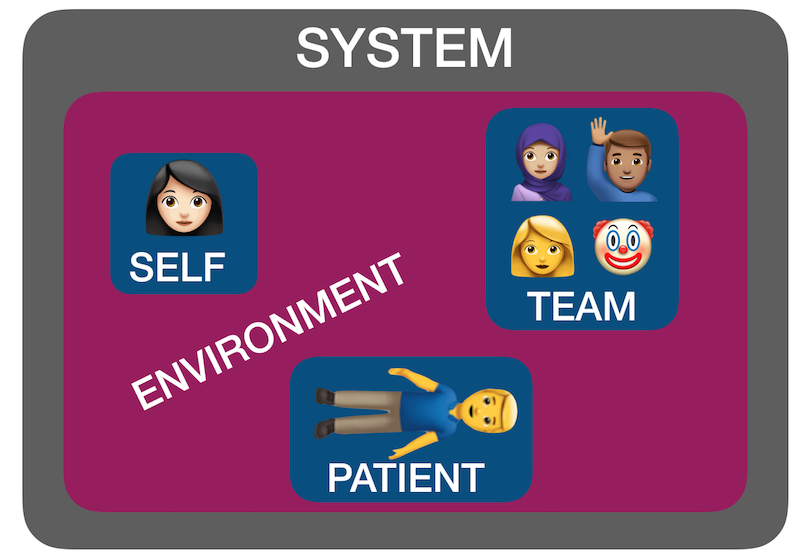
But ‘self, team, environment and patient’ isn’t just a useful system for case preparation. It can also be used for case analysis. I have found by discussing many ‘unsatisfactory’ cases over the years with participants in human factors workshops that STEP can help us identify where the issues lie. Accompanying all these factors is another ’S’: the system in which they interplay – the organisational rules, processes, policies, resources and deficiencies that may facilitate or obstruct an effective resuscitation(2).
Using STEPS to analyse cases The following (genuinely) hypothetical resus cases demonstrate how the application of this framework – Self, Team, Environment, Patient, System – might help identify correctible factors for future resuscitations:
1. Cardiac arrest in the bathroom on the orthopaedic ward – “it was chaos, there were too many people, and the resus trolley wasn’t properly stocked”.
STEPS analysis: Team – Leader needed to assign roles and allocate tasks Environment – Crowd control needed, lack of equipment System – Adequate checks for resus trolley not in place
2. 19-year-old male stabbed in the chest and arrested on arrival in hospital. CPR provided but went from PEA to asystole. Team leader discontinued resus after 20 minutes. Resident: “I thought he needed a resuscitative thoracotomy but no-one was willing to do it. No-one even mentioned it”.
STEPS analysis: Self – Lacked confidence to speak up, doubted own knowledge or influence Team – Lack of team situational awareness or knowledge or skill regarding required intervention System – Insufficient training and preparation for penetrating traumatic cardiac arrest scenario
3. 30-year-old mother with abdominal wound and her 2-year-old daughter with massive open head injury, both due to gunshot wounds, having been shot by husband/father who killed himself on scene. Child arrests in the ED, without ROSC, witnessed by mother before mother is taken to operating theatre.
STEPS analysis: Patient(s) – tragic case with upsetting circumstances and compounded psychological distress for patient and staff. The best resuscitation team in the world is not going to feel good about this one.
4. 46-year-old previously healthy male with VF arrest achieved ROSC after prehospital defibrillation and brought to the ED of a non-cardiac centre comatose and intubated. Further refractory VF in ED. Received multiple shocks, antiarrhythmics, double sequential external defibrillation. No on-site access to mechanical CPR, cardiac catheterisation, or ECMO. Patient declared dead in ED.
STEPS analysis: System – Prehospital team gave excellent care but brought the patient to a hospital ill-equipped to manage his ongoing needs, due to lack of ambulance service policy regarding appropriate destination hospital for cardiac arrest cases.
Summary You can see from the above cases how STEPS may be applied to make some sense of where a resus has gone wrong. Note that I am not recommending this as a way of structuring a team debrief or formal incident investigation – many institutions already have processes for conducting these and various rules and sensitivities have to be accommodated. Rather, this is a format I’ve found helpful in applying during informal discussions that aim to get the nub of where things could or should have gone better.
Occasionally, you can get a case where the STEPS seem to be aligned but things still feel bad – in which the outcome was unsatisfactory because the plan was wrong, or the team wasn’t able to execute the plan. In my next post I’ll discuss another way of analysing cases that can accompany STEPS.
AS A MEMBER OF THE MEDICAL PROFESSION:
I SOLEMNLY PLEDGE to dedicate my life to the service of humanity;
THE HEALTH AND WELL-BEING OF MY PATIENT will be my first consideration;
I WILL RESPECT the autonomy and dignity of my patient;
I WILL MAINTAIN the utmost respect for human life;
I WILL NOT PERMIT considerations of age, disease or disability, creed, ethnic origin, gender, nationality, political affiliation, race, sexual orientation, social standing, or any other factor to intervene between my duty and my patient;
I WILL RESPECT the secrets that are confided in me, even after the patient has died;
I WILL PRACTISE my profession with conscience and dignity and in accordance with good medical practice;
I WILL FOSTER the honour and noble traditions of the medical profession;
I WILL GIVE to my teachers, colleagues, and students the respect and gratitude that is their due;
I WILL SHARE my medical knowledge for the benefit of the patient and the advancement of healthcare;
I WILL ATTEND TO my own health, well-being, and abilities in order to provide care of the highest standard;
I WILL NOT USE my medical knowledge to violate human rights and civil liberties, even under threat;
I MAKE THESE PROMISES solemnly, freely, and upon my honour.
Have you deviated from any of the above?
Can you resolve not to in future?
What help do you need from your employer or your colleagues to allow you to adhere to them?
Can you think of colleagues who might benefit from being shown this pledge?
Please reflect on this line:
I will attend to my own health, well-being, and abilities in order to provide care of the highest standard
It is ABSOLUTELY RIGHT to prioritise these so you can be maximally effective for your patients.
If there are changes you need to make in this area, make them.
“What’s your leadership style Cliff? How do you like to run the emergency department?”
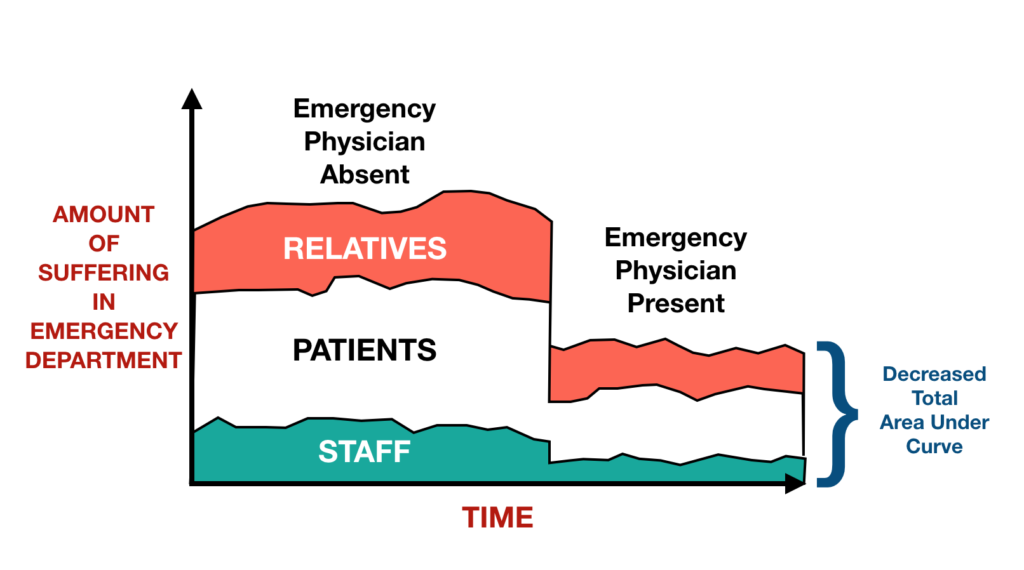
Our new fellow had asked a reasonable question. Although I’d never had to summarise it before, my reply came immediately: “I see my role as doing the most for the most by reducing the sum total of human suffering in the ED – both patients and staff”.
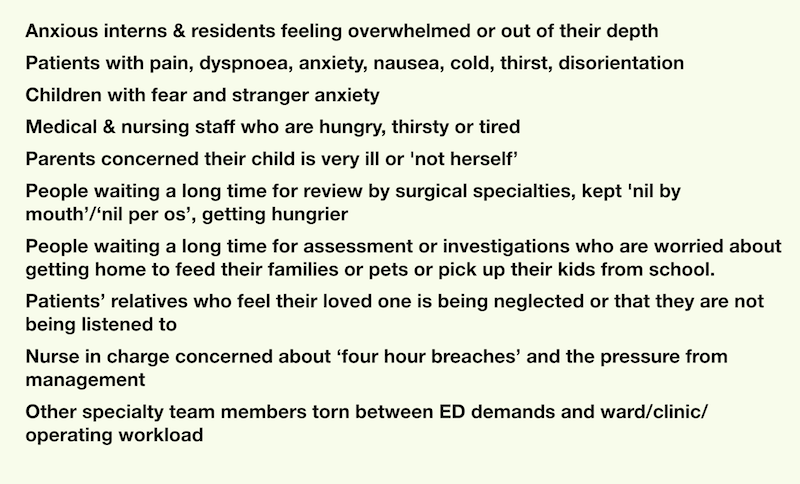
I hadn’t really reflected on this before. Obviously my clinical priority is resuscitation, but the reality is that resuscitation only contributes to a small proportion of ED workload. And when our resources and attention are prioritised to the resus room, the department fills with other patients in pain or distress, and their anxious relatives and parents(1).
Examples of the suffering, in patients, relatives, and staff, include:
Emergency departments really can be melting pots of human suffering, but there is so much we can do to reduce or relieve that suffering.
We just need to expand our view of our role from ‘diagnose and treat illness’ to ‘care for patients and their families’.
I believe an emergency physician can do much to reduce the ‘area under the curve’ – from listening to the nurses, buying a round of coffee, making sure rest breaks happen; to relieving pain, thirst and cold; to trying to prevent illness and injury from claiming someone’s loved ones; to being understanding to an admitting specialty colleague; to taking the time to explain to parents and relatives what is going on, and that you are taking their presentation seriously.
How I believe we can influence human suffering in the ED. This is a graphic to illustrate a concept, not a graph based on data.
I also believe this approach provides some protection from burnout.
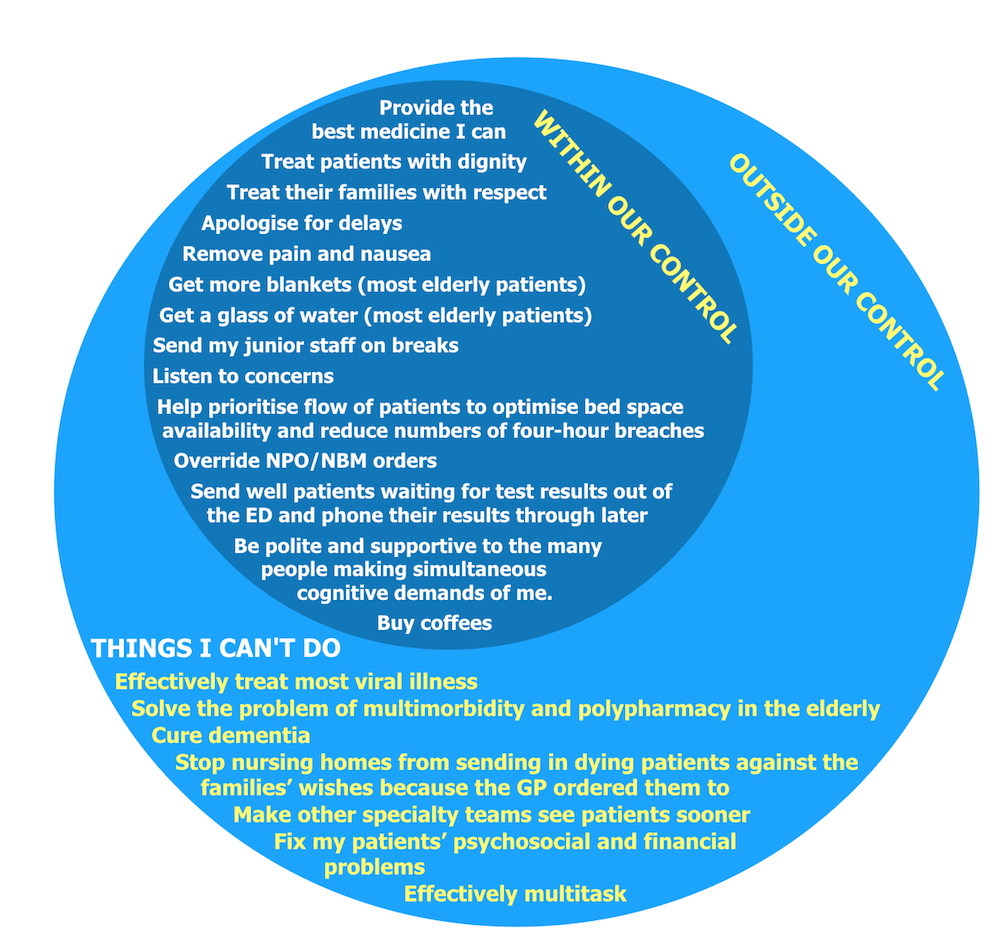
It is easy to be concerned with the difficult aspects of our job that are outside our control, which can result in stress and a sense of powerlessness. But there are so many things WITHIN our control that can make such a difference, that this is where our attention should focus.
This is the ‘Circle of Influence’ described by Steven Covey in “The 7 Habits of Highly Effective People”, in which he argues that the first habit, Proactivity, is demonstrated by people who work on problems within their circle of influence, rather than wasting time on those things outside it. Not only will this provide us with more satisfaction and sustainability in our career, it should also make us happier people, since expressing kindness for other people is a key component in the recipe for human happiness (which I describe here).
Of course, the other staff can also make a massive difference. However as the emergency physician clinically in charge of the floor, I have a responsibility to lead by example, and can exert far greater influence than more junior staff. As summarised recently by Liz Crowe and colleagues(2):
“EM doctors as the leads of the ED often set the ‘tone’ for the interdisciplinary staff within the team. Each EM doctor can choose to actively contribute to building a safe and supportive culture of collegial support, professional development and learning through high quality communication, humour and creating a sense of team within their departments.”
So let’s ALL set the tone. Support our teams, and show kindness to them and our patients. We can all help reduce the Area Under the Suffering Curve.
1. Body R, Kaide E, Kendal S, Foëx B. Not all suffering is pain: sources of patients’ suffering in the emergency department call for improvements in communication from practitioners. Emerg Med J. 2015 Jan;32(1):15–20.
This guest post from a fellow retrieval clinician contains a powerful message for us all. We have a responsibility to recognise the inevitability of clinician error, and to develop systems within our organisations to support those involved to avoid the ‘second victim’ phenomenon.
– 0:01: Error – Noun – A mistake
I was the picture perfect hire, I had tailored most of my career for our line of work: retrieval.
I was a senior FRU Paramedic with a background including the hottest terms: “clinical development”, “ultrasound”, “research”, “educator” and the useless alphabet soup that one inevitably acquires through enough time in healthcare. My CV was mint, printed on subtly thick paper to give a subliminal message of “excellence” – calculated moves for a calculated outcome.
I knew the protocols, policies, procedures before stepping through the door. With a fantastic orientation behind me, I was fucking awesome. I was in the stratosphere of awesome. Flightsuit, the smell of Jet A, podcasts blaring. I approached the one-year mark in retrieval feeling at home. Being granted complete clinical autonomy, I found my work deeply rewarding, stimulating. Nitric Oxide, ECMO, Ketamine, DSI/RSI, TXAblahblahblah. The buzz of Twitter was my daily work.
“Error” was a word, a noun. Error was a picture of crashed airplanes or derailed trains. Droning Powerpoints featured the Swiss cheese model and non-sequitur diagrams with abstract buzz-words. If you sucked, you crashed and burned. If you were good, you landed on the goddamn Hudson River.
+ 0:01: I am Error
Through an error in medication transitions, a young girl died under my care. Regardless of the slew of contributing factors, the latent errors – I am Proximate Cause. That is a title that is hard to shed. That is a title that follows you through day and night, wakefulness and sleep, at work, in the car, in the shower, in bed.
Having lost my desire to return to work, I drafted a curt letter of resignation and began the search for work elsewhere where I might be free of consequence. I was filled with dread waiting for my pager to go off, whispering a prayer for an easy tasking. I lacked the organizational or personal tools to process the slew of emotions I felt – incompetence, inadequacy and guilt. Just as easily as I had woven myself into who I was, I came undone.
+ 0:02: “Error-Free” – Adjective – Containing no mistakes
Despite our best attempts to adopt the lessons of aviation, aerospace and high-stakes systems into our craft, we in retrieval are primed for error throughout the work we do every day. We dive into the currents of diagnostic momentum, wading through the thoughts of others. The chaos swirling around us leads to erosion of situational awareness and the interruption of processes. The unforgiving physiology of the critically ill also force us to tread close to the edge. The margins are razor-thin, the consequences are great.
Just like we prepare for the risks involved with a complex machine such as the helicopter, we must train for the consequences of the complexities of medicine, such as error.
Our teams train for the very remote risk of over-water ditching through egress training yet little time is spent on a constant danger to our teams and our patients. The injection of simulated error through misdiagnoses, human factors and poorly labeled vials can not only prime the team for the capture of potential error but also the very real emotions that can result from mistakes – simulated or not. Much discussion has been had on resiliency training as of late, much of its focus on preparing teams for success in the midst of crisis. We must train for events such as an error like mine to prepare the individual clinician for the crisis that follows.
Yet the burden should not fall squarely on the individual clinician. As high performing organizations we have a duty to put in place transparent processes that can provide clinicians with support following a mistake as well as a clarity about “what comes next” following a mistake. As I consider my subsequent hardship following the death of this child, much of it took root in the lack of support from my organization and a lack of clarity about what would happen as a result of all this. More damaging than anything else is the solitude that comes with being unable to share one’s experience. A “second victim” left to their own devices to cope with their mistake is a victim of a system that has failed them.
We are equally primed for injury. One of your greatest strengths becomes your Achilles heel. We pursue our passions and find that resus and retrieval is the medicine that stimulates the cortex. This work inevitably becomes a fundamental part of who we are. The pursuit of excellence under the demanding conditions of our work is all-consuming, leading to this work become the very mesh of our being – “The Retrievalist” “The Resuscitationist.”
Following error, we experience an unraveling of who we are. The hard fall to the bottom is hard to recover from. I write this to let you know that it gets better and that you’re not alone. The resignation letter is deleted, the bottles stop emptying, the sleep comes more easily and you accept that in our craft, “error-free” is just a word, an adjective and that “error” is a noun and does not define you.
‘Do what you said you were going to do – the high performance culture of excellence under pressure’ is the title of a talk by General John Jansen, organised by my friend A/Prof Brian Burns on behalf of Sydney University.
It will be held on 20 December at 18.00 hrs at the Royal Prince Alfred Hospital in Sydney.
Free Registration available here, and refreshments are provided.
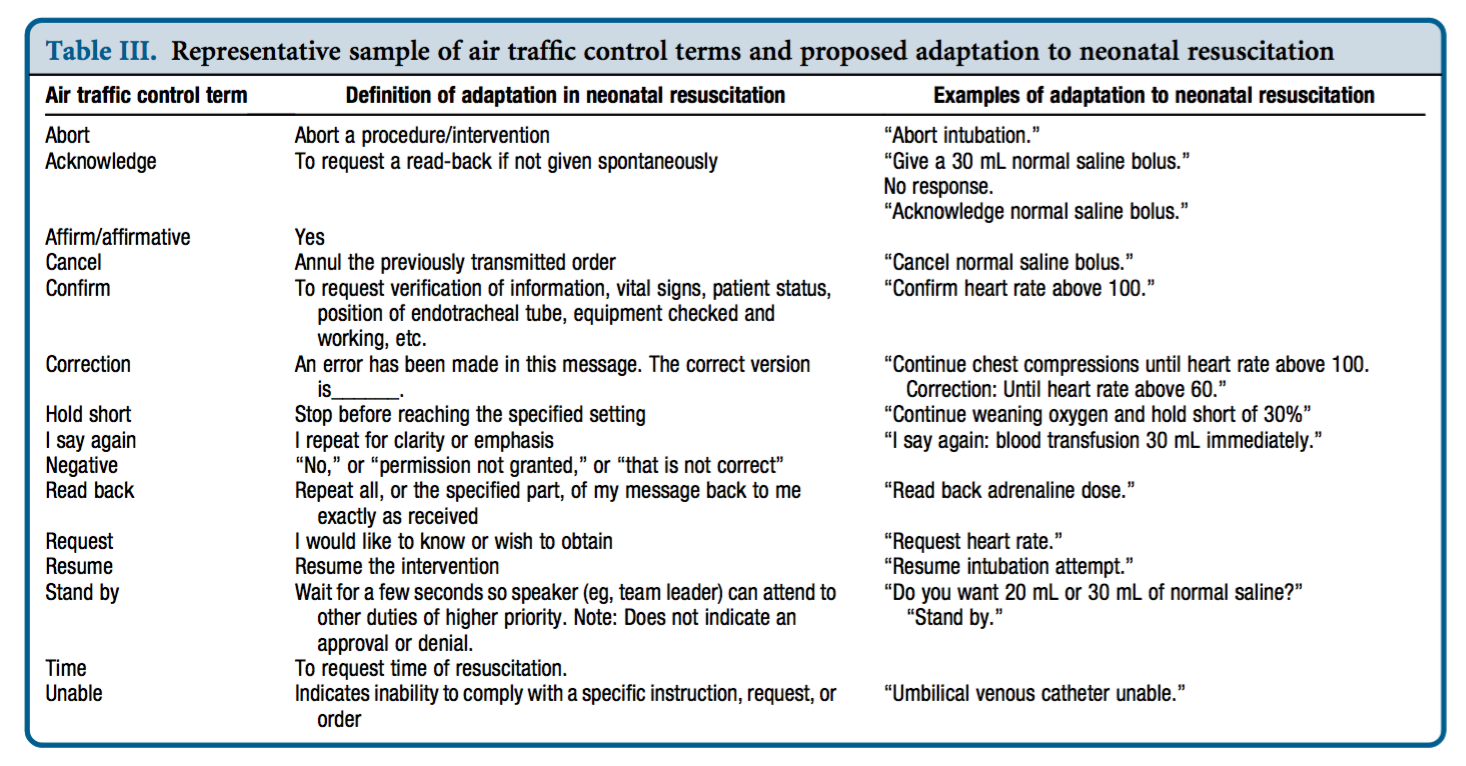
In the resus room, clarity of communication between team members is critical to patient safety and effective resuscitation. We are used to following standardised clinical algorithms for cardiac arrests and many other emergency presentations, but there is no standardisation of vocabulary or communication style. Communication failures are a major source of error in resuscitation, suggesting this is an area in which we need to improve.
Defining your lexicon
A contrast with the aviation industry was drawn by neonatologist Dr Nicole Yamada, who points out that pilots and air traffic controllers use an effective, concise, standardised set of words and phrases that are universally understood, for example ‘stand by’, ‘unable’, ‘read back’, and ‘cancel'(1). She proposed adapting a similar resuscitation-specific lexicon modelled after aviation communication which ‘would aid in streamlining communication during time-pressured clinical situations when seconds count and errors can kill.‘(2)
Dr Yamada tested this approach in a small study of simulated neonatal resuscitation. Standardised communication techniques were associated with a trend toward decreased error rate and faster initiation of critical interventions.(3)
Avoiding the fluff
In the absence of standardised approaches to communication, humans in the resus room often choose language which indirectly acknowledges social hierarchies. For ad hoc teams, phrases may be chosen which are least likely to offend people with whom we’re unfamiliar, or may be deferential in cases of real or presumed authority and expertise gradients. The consequence of this is the use of ‘mitigating language‘. Examples might be:
“Any chance you could pop a line in?”
“Would someone mind letting me know if they can feel a pulse?”
“Do you want to have a think about setting up for intubation?”
“How about we get some bag-mask ventilation happening at some point?”
“If you could have a look at his abdomen that would be awesome”
These commands (imperatives) phrased obliquely as questions or suggestions are know as ‘whimperatives‘ and are found throughout resus room dialogue, when the team leader does not wish to convey the assumption of a power relationship over her colleagues. These whimperatives are an example of ‘mitigating speech’, which refers to language that ‘de-emphasises’ or ‘sugarcoats’ the command.
‘The danger of mitigating language illustrates why, during medical crises, we should replace comments such as “perhaps, we need a surgeon” or “we should think about intubating” with “get me a surgeon” and “intubate the patient now.”’(4)
Conclusion
There’s nothing wrong with being polite and respectful, and mitigating language may be helpful in the team building phase. However the more critical the situation, the more an authorative/directive leadership style that clearly delegates critical tasks is required(5). Standardised terminology (with closed loop communication) is likely to enhance clarity of the message and accelerate the sharing of a team mental model. Avoiding whimperatives and excessive mitigating phrases may further prevent ambiguity and imprecision, reducing the time to critical interventions.
These components of the content of resus room communication – unequivocal, standardised, and direct – should go hand in hand with the delivery of the words. Effective delivery requires optimal delivery speed and ‘command presence’. These factors will be discussed in a future post.
I’d be interested to hear what standard phrases or words you think should be in the resus-room lexicon.
3. Yamada NK, Fuerch JH, Halamek LP. Impact of Standardized Communication Techniques on Errors during Simulated Neonatal Resuscitation. Am J Perinatol. 2016 Mar;33(4):385–92.
5. Bristowe KK, Siassakos DD, Hambly HH, Angouri JJ, Yelland AA, Draycott TJT, et al. Teamwork for clinical emergencies: interprofessional focus group analysis and triangulation with simulation. Qual Health Res. 2012 Sep 30;22(10):1383–94.
Last weekend I got my butt handed to me and I’m feeling really good about it. I entered my first Brazilian Jiu Jitsu competition, and was beaten unequivocally, having had to submit to avoid having my arm broken after about three minutes into the fight. So what’s to be so cheerful about? Essentially, the whole endeavour was an experiment, and the experiment was a success. I learned a heap about learning, and about myself. Lessons that can be applied to learning resuscitation medicine, or learning anything.
The 10000 hours fallacy: not all hours are created equal
I’ve been doing Brazilian Jiu Jitsu (BJJ) for about a year, and am not very good at it. I started it because my (then) five year old son started it, and I thought it would be nice if we could share an interest in something healthful and useful for self protection. For most of that year I made 1-2 sessions a week, usually rushing to class after an emergency department or retrieval medicine shift and not really having my ‘head in the game’. Turning up. Just like it’s possible to turn up to work, get through your shift, and go home and forget about it.
I noticed something interesting about the people who started around the same time as me. Those who were entering competitions – as inexperienced and ill-prepared as they were in the beginning – progressed much faster than me. They would break down techniques and work on specific movements or positions they knew they needed to improve because of their competition experience, and they’d ask targeted questions of the coaches, aimed at maximising feedback for them to work on. It dawned on me that I was witnessing something I’d described in a lecture on Cutting Edge Resuscitation performance at the Royal College of Emergency Medicine Conference last year:
“What seems to be apparent is that although many hours of practice are important, pure exposure or experience alone does not predict those who will master their subject. We may have all encountered colleagues who have many years under their belt who lack that spark you’d expect of a cutting edge expert. So merely turning up to work every day doesn’t make you better, it just makes you older. You reach a certain level where you can manage the majority of cases comfortably, after which more exposure to the same experience fails to improve performance expertise.
What differentiates the cutting edge performers from the majority in all these domains (studied areas such as chess or sports or music) appears to be the amount of deliberate practice, or effortful practice, in which individuals engage in tasks with the explicit goal of improving a particular aspect of performance, and continue to practice and modify their performance based on feedback, which can come from a coach or mentor or the results of the performance itself.”
“Competence does not equal excellence” – Weingart
With this realisation, I decided to enter a competition I was extremely unlikely to win. I knew that committing (publicly) to a deadline would force me to improve my game, and I turned up more, studied the notes I’d made, and started asking more questions. In the space of a few weeks I felt that my BJJ was progressing faster than before.
The powerful combined forces of deadlines and public commitment
There’s nothing like a deadline or a high stakes test or exam to focus the mind. I’ve done several postgraduate fellowships and diplomas by examination, some of which were optional, and I’m sure each one raised my knowledge and clinical ‘game’ more than any other educational intervention I can think of.
The reality of the competition day approaching forced me to tackle my training, fitness, diet and timetable in a way I otherwise would not have found the motivation for. I had a strange moment when I took off my teeshirt in the changing rooms prior to the match and caught sight of my reflection in the mirror. I barely recognised how different my physique was compared with months earlier. Previously, I’d exercised for its own sake and not made much progress losing the middle aged paunch. But the public commitment to a BJJ fight, in a certain weight category, instilled the drive to exercise and monitor my diet. Commitment to this deadline physically restructured me!
Stress exposure training WORKS!
I’ll be 49 this year. The only people available in my weight category to fight me were aged 36-40. Age can make a big difference. Injuries are not uncommon and a significant one could put me out of training or out of work. My wife and son and friends were going to watch me, and I didn’t want to let them down or put on a pathetic performance. All my buddies who had competed before warned me of the overwhelming nervousness that can disorientate you and cloud your concentration. There were plenty of potential negative outcomes to focus on, but I ignored them all. I knew the simple formula. Breathe. Talk. See.
This basic mantra, assisted by the mnemonic ‘Beat The Stress’ (BTS) developed by Michael Lauria, is something we teach and apply in the training department of Sydney HEMS. Breathe means control and pay attention to your breathing, allowing you to reduce sympathetic hyperactivation and be ‘in the moment’. Talk means positive self-talk: a silent internal monologue that reminds yourself of all the preparation you’ve done and the potential positive outcomes of the task about to be performed. See means visualise: run through in your mind a successful performance, imagining yourself overcoming any anticipated obstacles – a practice which prepares your mind and body for effective task execution.
Less than a week ago I was running workshops on human factors for Sydney University Masters of Medicine (Critical Care) students, and covered how we submit our new HEMS clinicians to stress exposure training in order for them to practice Lauria’s BTS approach. Throughout these workshops I couldn’t wait for the opportunity to test what I teach.
On the day, my only interpretation of my adrenal surge was excitement. Even in the ‘holding pen’ after weigh-in where you wait with other competitors to have your bout, there was no anxiety, no fear. I couldn’t wait to get on the mat. The whole thing was an exhilarating buzz, and even when the can of whoopass was being unloaded on me I felt cognitively ‘available’: aware of my surroundings (and predicament!) and able to control my breathing while I self-talked my way through my limited and ever dwindling options.
Conclusion
It might be slightly unusual to be singing from the rooftops about a defeat, but the educational principles I’m re-learning are worth re-sharing. I took myself out of a comfort zone, and made a public commitment to be tested. This focused my learning and made me practice in a different way and more proactively seek feedback. I no longer was ‘turning up’, I was training towards a goal. This renewed sense of ownership of my training transformed my level of engagement in the learning process, instilling an enthusiasm and craving to understand and test principles rather than rote learn techniques. I had an opportunity to test ‘Beat The Stress’ in a non-clinical setting and this mindware tool proved itself yet again. And despit
e the uninspiring outcome on the day, I was back sparring the following evening, with an even greater hunger for specific answers from the coaches, and with senior students remarking ‘you’ve got better’.
“It’s better to have it and not need it, than to need it and not have it“
My great friend and fellow Brit Lee Morrison is in Sydney again, teaching people how to save lives. Like a resuscitationist. But Lee isn’t a health care worker. He is a professional self protection instructor and martial athlete. The lives he is teaching people to save are their own and those of their friends and families. Lee has travelled the world and taught a diverse range of professionals including law enforcement and military special forces personnel. His current world tour will include the Czech Republic, USA, France, Russia and Germany after Australia.
What does this have to do with resuscitation? In my experience, almost everything. Hitting someone in self defence is technically very easy. Doing a resuscitative hysterotomy is technically very easy. Being able to do either of those things under stress can be difficult or impossible for some people.
Those who strive to understand and cultivate the Mind of the Resuscitationist know the importance of preparation through simulation under stress; the need to acknowledge and control the physiological and emotional response to stress; the necessity to train outside ones comfort zone and minimise the gap between simulated and real situations by optimising the cognitive fidelity of training scenarios; and the requirement to access the right mental state in an instant in which failure is not considered to be an option.
People who do not wish to witness the discussion or demonstration of violence or who cannot stand swearing should stop now. Those of you who want to see mastery in action watch the video below of Lee teaching in Germany.
I want you to appreciate the following:
Presentation style – how to connect with an audience and fully engage them through humour, passion, emphasis, intelligent discourse, and detailed explanations that connect emotionally and physically as well as intellectually.
The loss of fine motor skill under stress (2 min 13 sec)
The mindset of determination (2 min 48 sec) – consider how this relates to the perspective of the resuscitationist prepared to do a resuscitative thoracotomy under stress
How to influence and win arguments in a conflict situation by being assertive but providing a face-saving get-out for the aggressor. I have applied this multiple times in the resus room and in retrieval situations. (4 min 11 sec)
Training honestly – maintaining safety but ‘doing it like you f—-ing mean it’. Get out of your comfort zone and make the discomfort as real as possible. (7 min 37 sec)
How to minimise the gap between your training and what you’re training for, when legal, moral, and safety restrictions prevent you from doing the actual task for real as a training exercise. Using fatigue, pain, and disorientation as perturbations so you learn to recognise and mitigate their effects. (9 min 19 sec)
Accessing a single mental state that provides focus and prevents distraction from discomfort (11 min 40 sec)
If the video made you feel uncomfortable ask yourself why. If it’s because you consider yourself to be above violence and find the subject matter, language, and humour to be distasteful, that’s your right to feel like that. But try to dig a little deeper and ask yourself whether there are potential situations in your life that could confront you with fear or pain that you could be better prepared for if you trained with a different mindset.
When the situation arises that demands life-saving action and you are tired, hungry, scared, and discouraged by opposing advice or opinion, do you have the self-knowledge and resilience to see it through? If you don’t know the answer to that, isn’t it time you found out?
You can find out more about Lee at Urban Combatives




 “What’s your leadership style Cliff? How do you like to run the emergency department?”
“What’s your leadership style Cliff? How do you like to run the emergency department?”


 ‘Do what you said you were going to do – the high performance culture of excellence under pressure’ is the title of a talk by General John Jansen, organised by my friend
‘Do what you said you were going to do – the high performance culture of excellence under pressure’ is the title of a talk by General John Jansen, organised by my friend