We know that subarachnoid haemorrhage (SAH) can cause cardiac arrest. Some questions we may have about this are:
Questions
- What proportion of out-of-hospital cardiac arrests (OOHCA) who achieve return of spontaneous circulation (ROSC) are caused by SAH?
- What is the usual presenting arrest rhythm – VT/VF or non-shockable rhythms?
- What is the outcome of these patients – do any survive?
- Do they have other characteristic cardiac features, such as ECG or echo abnormalities?
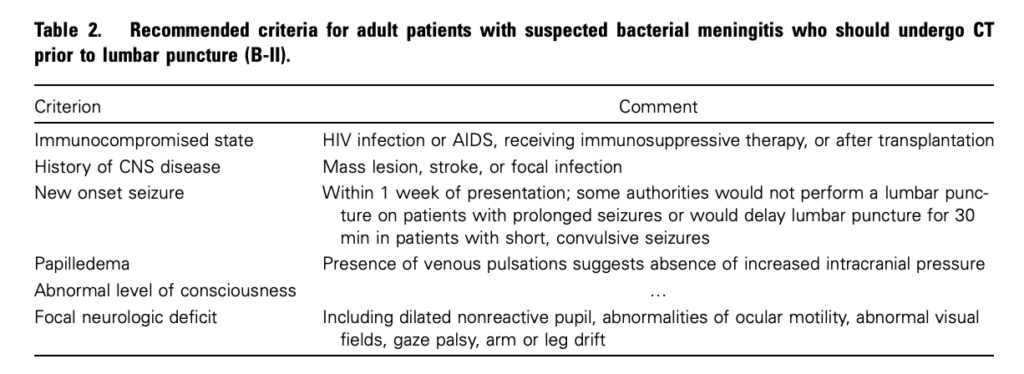
- Should we do a head CT on all survivors of out-of-hospital cardiac arrest of uncertain aetiology?
A recent Japanese article in Resuscitation1 is the third from that country to be published on the topic in three years, the other two2,3 coming from different centres and all demonstrating some consistent answers, as do papers published in recent years from Europe4 and North America5:
Answers
- Rates of SAH in OOHCA patients who achieve ROSC and make it to CT range from 4-16% (even higher if other sources of intracranial haemorrhage are included).
- Studies consistently demonstrate VT/VF to be very rare – PEA and asystole are by far the commonest presenting arrest rhythms.
- Almost no patients with this presentation due to SAH survive to hospital discharge.
- In the most recent study, all patients who survived long enough to get a 12 lead showed ST-T abnormalities and/or QT prolongation, although echocardiograms were mostly normal.
- Rates of SAH in OOHCA patients who achieve ROSC seem to be sufficiently high to seriously consider head CT in these patients if there is no obvious alternate explanation for the arrest.
1. Clinical and cardiac features of patients with subarachnoid haemorrhage presenting with out-of-hospital cardiac arrest
Resuscitation. 2011 Oct;82(10):1294-7
[EXPAND Abstract]
Background Subarachnoid haemorrhage (SAH) is known as one of the aetiologies of out-of-hospital cardiac arrest (OHCA). However, the mechanisms of circulatory collapse in these patients have remained unclear.
Methods and results We examined 244 consecutive OHCA patients transferred to our emergency department. Head computed tomography was performed on all patients and revealed the existence of SAH in 14 patients (5.9%, 10 females). Among these, sudden collapse was witnessed in 7 patients (50%). On their initial cardiac rhythm, all 14 patients showed asystole or pulseless electrical activity, but no ventricular fibrillation (VF). Return of spontaneous circulation (ROSC) was obtained in 10 of the 14 patients (14.9% of all ROSC patients) although all resuscitated patients died later. The ROSC rate in patients with SAH (71%) was significantly higher than that of patients with either other types of intracranial haemorrhage (25%, n = 2/8) or presumed cardiovascular aetiologies (22%, n = 23/101) (p < 0.01). On electrocardiograms, ST-T abnormalities and/or QT prolongation were found in all 10 resuscitated patients. Despite their electrocardiographic abnormalities, only 3 patients showed echocardiographic abnormalities.
Conclusions The frequency of SAH in patients with all causes of OHCA was about 6%, and in resuscitated patients was about 15%. The initial cardiac rhythm revealed no VF even though half had a witnessed arrest. A high ROSC rate was observed in patients with SAH, although none survived to hospital discharge.
[/EXPAND]
2. Assessing outcome of out-of-hospital cardiac arrest due to subarachnoid hemorrhage using brain CT during or immediately after resuscitation
Signa Vitae 2010; 5(2): 21 – 24 Full Text
[EXPAND Abstract]
Objectives. The clinical course and outcome of out-of-hospital cardiopulmonary arrest (OHCPA) due to subarachnoid hemorrhage (SAH) is unclear. The objective of this study is to clarify them.
Study design. Single- center, observational study. Setting. We usually perform a brain computed tomography (CT) in OHCPA patients who present without a clear etiology (42% of all OHCPA), such as trauma, to determine the cause of OHCPA and to guide treatment.
Patients. The study included OHCPA patients without a clear etiology, who were transferred to our center and who underwent a brain CT during resuscitation.
Methods of measurement. Patients’ records were reviewed; initial cardiac rhythm, existence of a witness and bystander cardiopulmonary resuscitation efforts (CPR) were compared with patients’ outcomes.
Results. Sixty-six patients were enrolled. 72.7% achieved return of spontaneous circulation (ROSC), 71.2% were admitted, 30.3% survived more than 7 days, and 9.1. survived-to-discharge. In 41 witnessed OHCPA, 87.8% obtained ROSC, 85.4% were admitted, and 14.6% survived-to-discharge. All survivors were witnessed. In 25 non-witnessed OHCPA, 48% obtained ROSC and were admitted, and no patients were discharged. Initial cardiac rhythm was ventricular fibrillation (VF), pulseless electrical activity (PEA) and asystole in 3.0%, 39.4%, and 47.0%. In 2 VF patients 50.0% survived-to- discharge, and there was no survivor with PEA or asystole.
Conclusion. This study shows a high rate of ROSC and admission in OHCPA patients with a SAH, and also reveals their very poor neurological outcome. We conclude that the detection of a SAH in OHCPA patients is important to determine the accurate frequency of SAH in this patient group and to guide appropriate treatment of all OHCPA patients.
[/EXPAND]
3. Subarachnoid haemorrhage as a cause of out-of-hospital cardiac arrest: A prospective computed tomography study
Resuscitation. 2009 Sep;80(9):977-80
[EXPAND Abstract]
Aim Aneurysmal subarachnoid haemorrhage (SAH) is a relatively common cause of out-of-hospital cardiac arrest (OHCA). Early identification of SAH-induced OHCA with the use of brain computed tomography (CT) scan obtained immediately after resuscitation may help emergency physicians make therapeutic decision as quickly as they can.
Methods During the 4-year observation period, brain CT scan was obtained prospectively in 142 witnessed non-traumatic OHCA survivors who remained haemodynamically stable after resuscitation. Demographics and clinical characteristics of SAH-induced OHCA survivors were compared with those with “negative” CT finding.
Results Brain CT scan was feasible with an average door-to-CT time of 40.0min. SAH was found in 16.2% of the 142 OHCA survivors. Compared with 116 survivors who were negative for SAH, SAH-induced OHCA survivors were significantly more likely to be female, to have experienced a sudden headache, and trended to have achieved return of spontaneous circulation (ROSC) prior to arrival in the emergency department less frequently. Ventricular fibrillation (VF) was significantly less likely to be seen in SAH-induced than SAH-negative OHCA (OR, 0.06; 95% CI, 0.01–0.46). Similarly, Cardiac Trop-T assay was significantly less likely to be positive in SAH-induced OHCA (OR, 0.08; 95% CI, 0.01–0.61).
Conclusion Aneurysmal SAH causes OHCA more frequently than had been believed. Immediate brain CT scan may particularly be useful in excluding SAH-induced OHCA from thrombolytic trial enrollment, for whom the use of thrombolytics is contraindicated. The low VF incidence suggests that VF by itself may not be a common cause of SAH-induced OHCA.
[/EXPAND]
4. Spontaneous subarachnoid haemorrhage as a cause of out-of-hospital cardiac arrest
Resuscitation. 2001 Oct;51(1):27-32
[EXPAND Abstract]
Objective: Spontaneous subarachnoid haemorrhage as a cause of out-of-hospital cardiac arrest is poorly evaluated. We analyse disease-specific and emergency care data in order to improve the recognition of subarachnoid haemorrhage as a cause of cardiac arrest.
Design: We searched a registry of cardiac arrest patients admitted after primarily successful resuscitation to an emergency department retrospectively and analysed the records of subarachnoid haemorrhage patients for predictive features.
Results: Over 8.5 years, spontaneous subarachnoidal haemorrhage was identified as the immediate cause in 27 (4%) of 765 out-of-hospital cardiac arrests. Of these 27 patients, 24 (89%) presented with at least three or more of the following common features: female gender (63%), age under 40 years (44%), lack of co-morbidity (70%), headache prior to cardiac arrest (39%), asystole or pulseless electric activity as the initial cardiac rhythm (93%), and no recovery of brain stem reflexes (89%). In six patients (22%), an intraventricular drain was placed, one of them (4%) survived to hospital discharge with a favourable outcome.
Conclusions: Subarachnoid haemorrhage complicated by cardiac arrest is almost always fatal even when a spontaneous circulation can be restored initially. This is due to the severity of brain damage. Subarachnoid haemorrhage may present in young patients without any previous medical history with cardiac arrest masking the diagnosis initially.
[/EXPAND]
5. Cranial computed tomography in the resuscitated patient with cardiac arrest
Am J Emerg Med. 2009 Jan;27(1):63-7
[EXPAND Abstract]
Introduction The incidence of out-of-hospital and in-hospital cardiorespiratory arrest from all causes in the United States occurs not infrequently. Postresuscitation care should include the identification of the inciting arrest event as well as therapy tailored to support the patient and treat the primary cause of the decompensation. The application of one particular testing modality, cranial computed tomography (CT) of the head, has not yet been determined. We undertook an evaluation of the use of head CT in patients who were resuscitated from cardiac arrest.
Methods Prehospital (emergency medical services), ED, and hospital records were reviewed for patients of all ages with cardiorespiratory arrest over a 4-year period (July 1996-June 2000). Information regarding diagnosis, management, and outcome was recorded. The results of cranial CT, if performed, and any apparent resulting therapeutic changes were recorded. Patients with a known traumatic mechanism for the cardiorespiratory arrest were excluded.
Results A total of 454 patients (mean age 58.3 years with 60% male) with cardiorespiratory arrest were entered in the study with 98 (22%) individuals (mean age 58.5 years with 53% male) undergoing cranial CT. Arrest location was as follows: emergency medical services, 41 (42%); ED, 11 (11%); and hospital, 46 (47%). Seventy-eight (79%) patients demonstrated 111 CT abnormalities: edema, 35 (32%); atrophy, 24 (22%); extra-axial hemorrhage, 14 (13%); old infarct, 12 (11%); new infarct, 11 (10%); intraparenchymal hemorrhage, 6 (5%); skull fracture, 5 (4%); mass, 3 (2%); and foreign body, 1 (1%). Therapeutic and diagnostic alterations in care were made in 38 (39%) patients—35 abnormal and 3 normal CTs. The following alterations occurred: medication administration, 26; withdrawal of life support, 7; additional diagnostic study, 6; neurologic consultation, 6; and intracranial pressure monitoring. 4. No patient survived to discharge.
Conclusion In this subset of resuscitated patients with cardiac arrest, abnormalities on the head CT were not uncommon. Alterations in management did occur in those patients with abnormalities. The indications and impact of head CT in the population of resuscitated patients with cardiac arrest remain unknown, warranting further investigation.
[/EXPAND]