A study of nonshockable out of hospital cardiac arrest survival showed significant improvement in short- and long-term survival and neurological outcome after implementation of a protocol consistent with CPR guidelines that prioritised chest compressions. These improvements were especially evident among arrests attributable to a cardiac cause, although there was no evidence of harm among arrests attributable to a noncardiac cause.
This was not a randomised trial so unrecognised factors may have contributed to the improved outcome in addition to the change in CPR protocol. However, it is interesting as it provides up to date survival rates from a large population sample: Non shockable out of hospital cardiac arrests achieve return of spontaneous circulation in 34%, 6.8% are discharged from hospital (5.1% with a favourable neurological outcome), and 4.9% survived one year.
The breakdown between PEA and asystole is of course telling, and unsurprising, with 12.8% versus 1.1% being discharged with a favourable neurological outcome, respectively. I would imagine then that some of the PEA patients had beating hearts with hypotension extreme enough to cause pulselessness (pseudo-electromechanical dissociation) – clinically a ‘cardiac arrest’ but really nothing of the sort, and the reason we use cardiac ultrasound to prognosticate.
BACKGROUND: Out-of-hospital cardiac arrest (OHCA) claims millions of lives worldwide each year. OHCA survival from shockable arrhythmias (ventricular fibrillation/ tachycardia) improved in several communities after implementation of American Heart Association resuscitation guidelines that eliminated “stacked” shocks and emphasized chest compressions. “Nonshockable” rhythms are now the predominant presentation of OHCA; the benefit of such treatments on nonshockable rhythms is uncertain.
METHODS AND RESULTS: We studied 3960 patients with nontraumatic OHCA from nonshockable initial rhythms treated by prehospital providers in King County, Washington, over a 10-year period. Outcomes during a 5-year intervention period after adoption of new resuscitation guidelines were compared with the previous 5-year historical control period. The primary outcome was 1-year survival. Patient demographics and resuscitation characteristics were similar between the control (n=1774) and intervention (n=2186) groups, among whom 471 of 1774 patients (27%) versus 742 of 2186 patients (34%), respectively, achieved return of spontaneous circulation; 82 (4.6%) versus 149 (6.8%) were discharged from hospital, 60 (3.4%) versus 112 (5.1%) with favorable neurological outcome; 73 (4.1%) versus 135 (6.2%) survived 1 month; and 48 (2.7%) versus 106 patients (4.9%) survived 1 year (all P≤0.005). After adjustment for potential confounders, the intervention period was associated with an improved odds of 1.50 (95% confidence interval, 1.29-1.74) for return of spontaneous circulation, 1.53 (95% confidence interval, 1.14-2.05) for hospital survival, 1.56 (95% confidence interval, 1.11-2.18) for favorable neurological status, 1.54 (95% confidence interval, 1.14-2.10) for 1-month survival, and 1.85 (95% confidence interval, 1.29-2.66) for 1-year survival.
CONCLUSION: Outcomes from OHCA resulting from nonshockable rhythms, although poor by comparison with shockable rhythm presentations, improved significantly after implementation of resuscitation guideline changes, suggesting their potential to benefit all presentations of OHCA.
Impact of changes in resuscitation practice on survival and neurological outcome after out-of-hospital cardiac arrest resulting from nonshockable arrhythmia Circulation. 2012 Apr 10;125(14):1787-94
A case is reported in Prehospital Emergency Care1 in which an agitated patient (due to mania and alcohol intoxication) received 5 mg/kg (500 mg) of ketamine intramuscularly by an EMS crew which dissociated him within a few minutes. He subsequently developed episodes of laryngospasm in the emergency department which were unrelieved by head tilt, chin lift and simple airway adjuncts but responded to bag-mask ventilation (BMV). The patient was intubated because the laryngospasm recurred, although it had again responded to BMV.
The authors make the point that because of the response of laryngospasm to simple manoeuvres, and because in the prehospital environment a patient will not be left without an EMS provider present, ‘restricting ketamine to EMS units capable of rapid-sequence intubation therefore seems unnecessary.‘
This is one for EMS directors to consider seriously. Personally, I think practicing prehospital care without access to ketamine is like having a hand tied behind my back. Ketamine opens up a world of possibilities in controlling combative patients, optimising scene safety, providing sedation for painful procedures including extrication, and enabling severe pain to be controlled definitively.
I’ve been using ketamine regularly for prehospital analgesia and emergency department procedural sedation in both adults and kids for more than a decade. I’ve seen significant laryngospasm 5 times (twice in kids). On one of those occasions, a 3 year old child desaturated to around 50% twice during two episodes of laryngospasm. We weren’t slow to pick it up – that was just her showing us how quickly kids can desaturate which continued while we went through a stepwise approach until BMV resolved it. It was however an eye opener for the registrar (senior resident) assisting me, who became extremely respectful of ketamine after that. Our ED sedation policy (that I wrote) required that suxamethonium was ready and available and that an appropriate dose had been calculated before anyone got ketamine. Paralysis may extremely rarely be required, but when it’s needed you need to be ready.
The best monitor for laryngospasm – noninvasive capnography
Laryngospasm is rare but most regular prescribers of ketamine will have seen it; the literature says it occurs in about 1-2% of sedations, although anecdotally I think it’s a bit less frequent. Importantly for those weighing the risks of allowing non-RSI competent prescribers, the requirement for intubation is exceptionally rare (2 of 11,589 reported cases in one review). Anyone interested should read this excellent review of ketamine-related adverse effects provided by Chris Nickson at Life in The Fast Lane. Chris reminds us of the Larson manouevre, which is digital pressure in the notch behind and below the ear, described by Larson2 as follows:
The technique involves placing the middle finger of each hand in what I term the laryngospasm notch. This notch is behind the lobule of the pinna of each ear. It is bounded anteriorly by the ascending ramus of the mandible adjacent to the condyle, posteriorly by the mastoid process of the temporal bone, and cephalad by the base of the skull. The therapist presses very firmly inward toward the base of the skull with both fingers, while at the same time lifting the mandible at a right angle to the plane of the body (i.e., forward displacement of the mandible or “jaw thrust”). Properly performed, it will convert laryngospasm within one or two breaths to laryngeal stridor and in another few breaths to unobstructed respirations.
I use this point most often to provide painful stimuli when assessing GCS in a patient, particular those I think may be feigning unconsciousness (I’ve done this for a number of years since learning how painful it can be when I was shown it by a jujitsu instructor). Dr Larson says he was taught the technique by Dr Guadagni, so perhaps we should be calling it the ‘Guadagni manouevre’. The lack of published evidence has led to some appropriate skepticism3, but as it can be combined with a jaw thrust it needn’t delay more aggressive interventions should they become necessary, it may work, and it’s likely to be harmless.
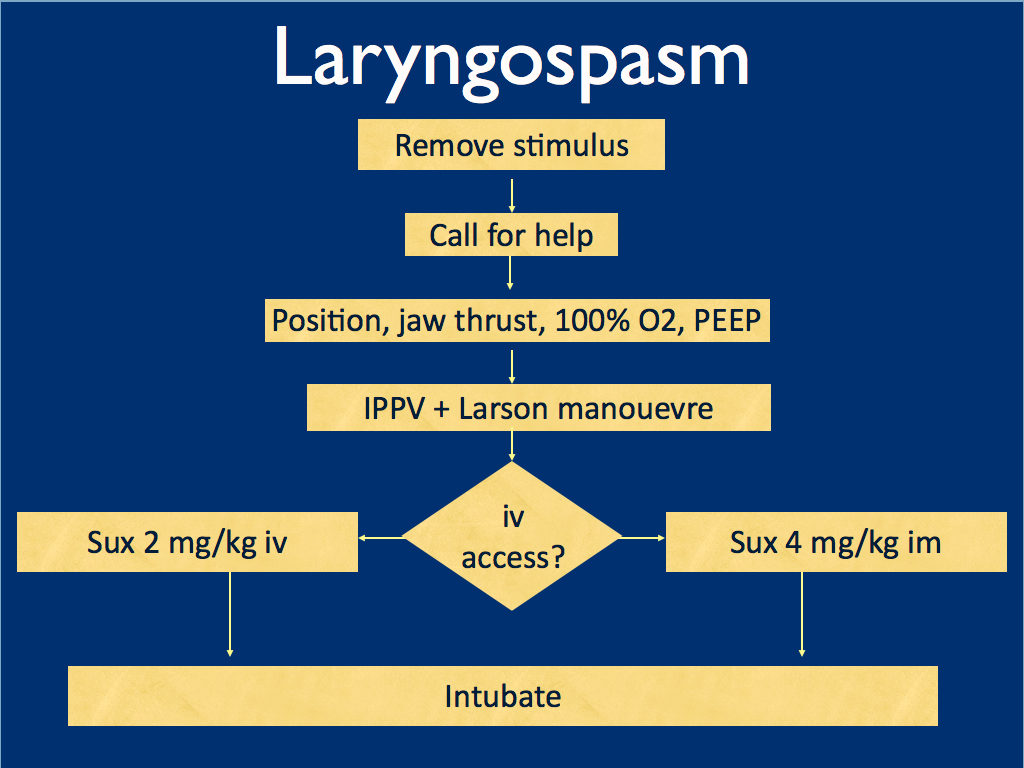
I presented the following suggested algorithm for management of laryngospasm during ketamine procedural sedation at a regional emergency medicine ‘Fellows Forum’ meeting in November 2007 in the UK. Since many paediatric procedural sedations were done using intramuscular (im) ketamine, it gives guidance based on whether or not vascular access has been obtained:
Some things I considered were:
Neuromuscular blockade (NMB) isn’t always necessary – laryngospasm may be managed with other sedatives such as propofol. However, titrating further sedatives in a desaturating child in my view is inferior to definitive airway management and laryngeal relaxation with suxamethonium and a tube.
Laryngospasm may be managed with much smaller doses of suxamethonium than are required for intubation – as little as 0.1 mg/kg may be effective. However, I think once we go down the NMB route we’re committed to intubation and therefore we should use a dose guaranteed to be effective in achieving intubating conditions.
In the child without vascular access, I considered intraosseous and intralingual sux. However, intramuscular suxamethonium is likely to have a relaxant effect on the laryngeal muscles within 30-45 seconds, which has to be compared with time taken to insert and confirm intraosseous needle placement. I do not think the traditionally recommended intralingual injection has any role to play in modern airway management.
At the time I wrote this most paediatric resuscitation bays in my area in the United Kingdom had breathing circuits capable of delivering PEEP – usually the Ayr’s T-Piece (specifically the Mapleson F system), which is why PEEP was included early in in the algorithm prior to BMV.
I have since modified it for two reasons: firstly, we might as well do the Larson manoeuvre during the jaw thrust; secondly, many Australasian and US EDs will only be able to deliver PEEP with a PEEP valve attached to a BVM, so PEEP has been moved to the BVM stage.
I would love to hear what people are doing in their prehospital and inhospital practice. Should ketamine only be administered by providers who can offer RSI? Do you have a laryngospasm protocol? If so, I’d love to see it. If not, feel free to use or adapt my unvalidated one at your own risk.
ABSTRACT An advanced life support emergency medical services (EMS) unit was dispatched with law enforcement to a report of a male patient with a possible overdose and psychiatric emergency. Police restrained the patient and cleared EMS into the scene. The patient was identified as having excited delirium, and ketamine was administered intramuscularly. Sedation was achieved and the patient was transported to the closest hospital. While in the emergency department, the patient developed laryngospasm and hypoxia. The airway obstruction was overcome with bag–valve–mask ventilation. Several minutes later, a second episode of laryngospasm occurred, which again responded to positive-pressure ventilation. At this point the airway was secured with an endotracheal tube. The patient was uneventfully extubated several hours later. This is the first report of laryngospam and hypoxia associated with prehospital administration of intramuscular ketamine to a patient with excited delirium.
This UK study showed that paramedics could successfully acquire and identify lung ultrasound images after a two day course. The course covered the identification and management of patients who present with serious thoracic injury, with a specific focus on the use of thoracic ultrasound during early prehospital assessment. Standard 2D images for pleural sliding and comet tails and M-Mode for the ‘seashore sign’ were acquired, and colour Doppler was also used to assist in the identification of pleural sliding.
Objective This trial investigated whether advanced paramedics from a UK regional ambulance service have the ability to acquire and interpret diagnostic quality ultrasound images following a 2-day programme of education and training covering the fundamental aspects of lung ultrasound.
Method The participants were tested using a two-part examination; assessing both their theoretical understanding of image interpretation and their practical ability to acquire diagnostic quality ultrasound images. The results obtained were subsequently compared with those obtained from expert physician sonographers.
Results The advanced paramedics demonstrated an overall accuracy in identifying the presence or absence of pneumothorax in M-mode clips of 0.94 (CI 0.86 to 0.99), compared with the experts who achieved 0.93 (CI 0.67 to 1.0). In two-dimensional mode, the advanced paramedics demonstrated an overall accuracy of 0.78 (CI 0.72 to 0.83), compared with the experts who achieved 0.76 (CI 0.62 to 0.86). In total, the advanced paramedics demonstrated an overall accuracy at identifying the presence or absence of pneumothorax in prerecorded video clip images of 0.82 (CI 0.77 to 0.86), in comparison
with the expert users of 0.80 (CI 0.68 to 0.88). All of the advanced paramedics passed the objective structured clinical examination and achieved a practical standard considered by the examiners to be equivalent to that which would be expected from candidates enrolled on the thoracic module of the College of Emergency Medicine level 2 ultrasound programme.
Conclusion This trial demonstrated that ultrasound-naive practitioners can achieve an acceptable standard of competency in a simulated environment in a relatively short period of time.
Acquisition and interpretation of focused diagnostic ultrasound images by ultrasound-naive advanced paramedics: trialling a PHUS education programme Emerg Med J, 2012 vol. 29 (4) pp. 322-326
A military study revealed troops suffering from severe burns tended to receive either no prehospital fluid or too much fluid1.
The authors point out some practical realities and an attempted solution:
For a medic potentially treating multiple casualties at once in a hostile environment, the calculation of the modified Brooke or Parkland formula may be unrealistic prior to beginning fluid resuscitation in the prehospital setting.
The USAISR’s Rule of 10 is a simplified formula to guide the initial fluid resuscitation of a burn victim. The burn size is estimated to the nearest 10% TBSA. For patients weighing 40 to 80 kg, the burn size is then multiplied by 10 to give the initial fluid rate in milliliters per hour. The rate is increased by 100 mL/hour for every 10 kg above 80 kg in terms of the patient’s weight. For the majority of adult burn patients, the Rule of 10 approximates the initial fluid rate within accepted ABA guidelines.
A previous study on the rule of 10 showed it provided an estimate that fell between the modified Brooke and Parkland estimates 87.8% of the time, less than the modified Brooke <12% of the time, and hardly ever (>1%) exceeded the Parkland estimate2.
OBJECTIVE: The purpose of this article is to provide a descriptive study of the management of burns in the prehospital setting of a combat zone.
METHODS: A retrospective chart review was performed of U.S. casualties with >20% total-body-surface-area thermal burns, transported from the site of injury to Ibn Sina Combat Support Hospital (CSH) between January 1, 2006, and August 30, 2009.
RESULTS: Ibn Sina CSH received 225 burn casualties between January 2006 and August 2009. Of these, 48 met the inclusion criteria. The mean Injury Severity Score was 31.7 (range 4 to 75). Prehospital vascular access was obtained in 24 casualties (50%), and 20 of the casualties received fluid resuscitation. Out of the 48 casualties enrolled, 28 (58.3%) did not receive prehospital fluid resuscitation. Of the casualties who received fluid resuscitation, nearly all received volumes in excess of the guidelines established by the American Burn Association and those recommended by the Committee for Tactical Combat Casualty Care. With regard to pain management in the prehospital setting, 13 casualties (27.1%) received pain medication.
CONCLUSIONS: With regard to the prehospital fluid resuscitation of primary thermal injury in the combat zone, two extremes were noted. The first group did not receive any fluid resuscitation; the second group was resuscitated with fluid volumes higher than those expected if established guidelines were utilized. Pain management was not uniformly provided to major burn casualties, even in several with vascular access. These observations support improved education of prehospital personnel serving in a combat zone.
In one of largest studies to date of prehospital capnography in cardiac arrest, an initial EtCO2 >10 mmHg (1.3 kPa) was associated with an almost five-fold higher rate of return of spontaneous circulation (ROSC). In addition, a decrease in the EtCO2 during resuscitative events of >25% was associated with a significant increase in mortality, independent of other variables known to affect outcome.
The authors conclude: “EtCO2 values should be included as important variables in protocols to terminate or continue resuscitation in the prehospital setting“.
OBJECTIVE: The objective of this study was to evaluate initial end-tidal CO2 (EtCO2) as a predictor of survival in out-of-hospital cardiac arrest.
METHODS: This was a retrospective study of all adult, non-traumatic, out-of-hospital, cardiac arrests during 2006 and 2007 in Los Angeles, California. The primary outcome variable was attaining return of spontaneous circulation (ROSC) in the field. All demographic information was reviewed and logistic regression analysis was performed to determine which variables of the cardiac arrest were significantly associated with ROSC.
RESULTS: There were 3,121 cardiac arrests included in the study, of which 1,689 (54.4%) were witnessed, and 516 (16.9%) were primary ventricular fibrillation (VF). The mean initial EtCO2 was 18.7 (95%CI = 18.2-19.3) for all patients. Return of spontaneous circulation was achieved in 695 patients (22.4%) for which the mean initial EtCO2 was 27.6 (95%CI = 26.3-29.0). For patients who failed to achieve ROSC, the mean EtCO2 was 16.0 (95%CI = 15.5-16.5). The following variables were significantly associated with achieving ROSC: witnessed arrest (OR = 1.51; 95%CI = 1.07-2.12); initial EtCO2 >10 (OR = 4.79; 95%CI = 3.10-4.42); and EtCO2 dropping <25% during the resuscitation (OR = 2.82; 95%CI = 2.01-3.97).The combination of male gender, lack of bystander cardiopulmonary resuscitation, unwitnessed collapse, non-vfib arrest, initial EtCO2 ≤10 and EtCO2 falling > 25% was 97% predictive of failure to achieve ROSC.
CONCLUSIONS: An initial EtCO2 >10 and the absence of a falling EtCO2 >25% from baseline were significantly associated with achieving ROSC in out-of-hospital cardiac arrest. These additional variables should be incorporated in termination of resuscitation algorithms in the prehospital setting.
This appears to be a useful option when iv access is difficult and the patient is relatively stable.
The protocol specified nebulisation of 2 mg of naloxone with 3 mL of normal saline as empiric treatment for suspected opioid overdose or undifferentiated depressed respirations as long as the patient had some spontaneous respiratory effort, no apnoea, and no severe cardiorespiratory compromise.
BACKGROUND: Emergency medical services (EMS) traditionally administer naloxone using a needle. Needleless naloxone may be easier when intravenous (IV) access is difficult and may decrease occupational blood-borne exposure in this high-risk population. Several studies have examined intranasal naloxone, but nebulized naloxone as an alternative needleless route has not been examined in the prehospital setting.
OBJECTIVE: We sought to determine whether nebulized naloxone can be used safely and effectively by prehospital providers for patients with suspected opioid overdose.
METHODS: We performed a retrospective analysis of all consecutive cases administered nebulized naloxone from January 1 to June 30, 2010, by the Chicago Fire Department. All clinical data were entered in real time into a structured EMS database and data abstraction was performed in a systematic manner. Included were cases of suspected opioid overdose, altered mental status, and respiratory depression; excluded were cases where nebulized naloxone was given for opioid-triggered asthma and cases with incomplete outcome data. The primary outcome was patient response to nebulized naloxone. Secondary outcomes included need for rescue naloxone (IV or intramuscular), need for assisted ventilation, and adverse antidote events. Kappa interrater reliability was calculated and study data were analyzed using descriptive statistics.
RESULTS: Out of 129 cases, 105 met the inclusion criteria. Of these, 23 (22%) had complete response, 62 (59%) had partial response, and 20 (19%) had no response. Eleven cases (10%) received rescue naloxone, no case required assisted ventilation, and no adverse events occurred. The kappa score was 0.993.
CONCLUSION: Nebulized naloxone is a safe and effective needleless alternative for prehospital treatment of suspected opioid overdose in patients with spontaneous respirations.
This small study on traumatic arrests in children1 refutes the “100% mortality from traumatic arrest” dogma that people still spout and gives information on the mechanisms associated with survival: drowning and strangulation were associated with greater rates of survival to hospital admission compared with blunt, penetrating, and other traumas. Overall, drowning had the greatest rate of survival to discharge (19.1%).
I would like to know the injuries sustained in non-survivors, to determine whether they were potentially treatable. Strikingly, in the list of prehospital procedures performed, there were NO attempts at pleural decompression, something that is standard in traumatic arrest protocols in prehospital services were I have worked.
It is interesting to compare these results with those of the London HEMS team2, who for traumatic paediatric arrest achieved 19/80 (23.8%) survival to discharged from the emergency department and 7/80 (8.75%) survival to hospital discharge. They also noted a large proportion of the survivors suffered hypoxic or asphyxial injuries, whereas those patients with hypovolaemic cardiac arrest did not survive.
OBJECTIVE:To determine the epidemiology and survival of pediatric out-of-hospital cardiac arrest (OHCA) secondary to trauma.
METHODS:The CanAm Pediatric Cardiac Arrest Study Group is a collaboration of researchers in the United States and Canada sharing a common goal to improve survival outcomes for pediatric cardiac arrest. This was a prospective, multicenter, observational study. Twelve months of consecutive data were collected from emergency medical services (EMS), fire, and inpatient records from 2000 to 2003 for all OHCAs secondary to trauma in patients aged ≤18 years in 36 urban and suburban communities supporting advanced life support (ALS) programs. Eligible patients were apneic and pulseless and received chest compressions in the field. The primary outcome was survival to discharge. Secondary measures included return of spontaneous circulation (ROSC), survival to hospital admission, and 24-hour survival.
RESULTS:The study included 123 patients. The median patient age was 7.3 years (interquartile range [IQR] 6.0-17.0). The patient population was 78.1% male and 59.0% African American, 20.5% Hispanic, and 15.7% white. Most cardiac arrests occurred in residential (47.1%) or street/highway (37.2%) locations. Initial recorded rhythms were asystole (59.3%), pulseless electrical activity (29.1%), and ventricular fibrillation/tachycardia (3.5%). The majority of cardiac arrests were unwitnessed (49.5%), and less than 20% of patients received chest compressions by bystanders. The median (IQR) call-to-arrival interval was 4.9 (3.1-6.5) minutes and the on-scene interval was 12.3 (8.4-18.3) minutes. Blunt and penetrating traumas were the most common mechanisms (34.2% and 25.2%, respectively) and were associated with poor survival to discharge (2.4% and 6.5%, respectively). For all OHCA patients, 19.5% experienced ROSC in the field, 9.8% survived the first 24 hours, and 5.7% survived to discharge. Survivors had triple the rate of bystander cardiopulmonary resuscitation (CPR) than nonsurvivors (42.9% vs. 15.2%). Unlike patients sustaining blunt trauma or strangulation/hanging, most post-cardiac arrest patients who survived the first 24 hours after penetrating trauma or drowning were discharged alive. Drowning (17.1% of cardiac arrests) had the highest survival-to-discharge rate (19.1%).
CONCLUSIONS:The overall survival rate for OHCA in children after trauma was low, but some trauma mechanisms are associated with better survival rates than others. Most OHCA in children is preventable, and education and prevention strategies should focus on those overrepresented populations and high-risk mechanisms to improve mortality.
Some defibrillators have accelerometers capable of measuring chest compression depth during CPR. This allowed a study correlating compression depth with survival in out of hospital cardiac arrest.
More than half of patients received less than the 2005 recommended chest compression depth of 38–51 mm and >90% received less than the 2010 recommended depth of >50 mm. There was an inverse relationship between rate and depth, ie. rescuers had a tendency to ‘push hard, push slow’ or ‘push soft, push fast’.
The authors state: We found an association between adequate compression depth and good outcomes but could not demonstrate that the 2010 recommendations are better than those from 2005. Although we believe that compression depth is an important component of CPR and should be measured routinely during cardiac arrest resuscitation, we believe that the optimal depth is currently unknown.
BACKGROUND: The 2010 international guidelines for cardiopulmonary resuscitation recently recommended an increase in the minimum compression depth from 38 to 50 mm, although there are limited human data to support this. We sought to study patterns of cardiopulmonary resuscitation compression depth and their associations with patient outcomes in out-of-hospital cardiac arrest cases treated by the 2005 guideline standards.
DESIGN: Prospective cohort.
SETTING: Seven U.S. and Canadian urban regions.
PATIENTS: We studied emergency medical services treated out-of-hospital cardiac arrest patients from the Resuscitation Outcomes Consortium Epistry-Cardiac Arrest for whom electronic cardiopulmonary resuscitation compression depth data were available, from May 2006 to June 2009.
MEASUREMENTS: We calculated anterior chest wall depression in millimeters and the period of active cardiopulmonary resuscitation (chest compression fraction) for each minute of cardiopulmonary resuscitation. We controlled for covariates including compression rate and calculated adjusted odds ratios for any return of spontaneous circulation, 1-day survival, and hospital discharge.
MAIN RESULTS: We included 1029 adult patients from seven U.S. and Canadian cities with the following characteristics: Mean age 68 yrs; male 62%; bystander witnessed 40%; bystander cardiopulmonary resuscitation 37%; initial rhythms: Ventricular fibrillation/ventricular tachycardia 24%, pulseless electrical activity 16%, asystole 48%, other nonshockable 12%; outcomes: Return of spontaneous circulation 26%, 1-day survival 18%, discharge 5%. For all patients, median compression rate was 106 per minute, median compression fraction 0.65, and median compression depth 37.3 mm with 52.8% of cases having depth <38 mm and 91.6% having depth <50 mm. We found an inverse association between depth and compression rate ( p < .001). Adjusted odds ratios for all depth measures (mean values, categories, and range) showed strong trends toward better outcomes with increased depth for all three survival measures.
CONCLUSIONS: We found suboptimal compression depth in half of patients by 2005 guideline standards and almost all by 2010 standards as well as an inverse association between compression depth and rate. We found a strong association between survival outcomes and increased compression depth but no clear evidence to support or refute the 2010 recommendations of >50 mm. Although compression depth is an important component of cardiopulmonary resuscitation and should be measured routinely, the most effective depth is currently unknown.
A large retrospective study has shown increased trauma survival associated with helicopter transport. The reason is unclear and may be multifactorial: faster speed, greater access to trauma centres, higher exposure of crews to trauma, different crew skill mix and so on are all possibilities.
An interview of less than five minutes with one of the authors describes the study:
Context Helicopter emergency medical services and their possible effect on outcomes for traumatically injured patients remain a subject of debate. Because helicopter services are a limited and expensive resource, a methodologically rigorous investigation of its effectiveness compared with ground emergency medical services is warranted.
Objective To assess the association between the use of helicopter vs ground services and survival among adults with serious traumatic injuries.
Design, Setting, and Participants Retrospective cohort study involving 223 475 patients older than 15 years, having an injury severity score higher than 15, and sustaining blunt or penetrating trauma that required transport to US level I or II trauma centers and whose data were recorded in the 2007-2009 versions of the American College of Surgeons National Trauma Data Bank.
Interventions Transport by helicopter or ground emergency services to level I or level II trauma centres.
Main Outcome Measures Survival to hospital discharge and discharge disposition.
Results A total of 61 909 patients were transported by helicopter and 161 566 patients were transported by ground. Overall, 7813 patients (12.6%) transported by helicopter died compared with 17 775 patients (11%) transported by ground services. Before propensity score matching, patients transported by helicopter to level I and level II trauma centers had higher Injury Severity Scores. In the propensity score–matched multivariable regression model, for patients transported to level I trauma centers, helicopter transport was associated with an improved odds of survival compared with ground transport (odds ratio [OR], 1.16; 95% CI, 1.14-1.17; P < .001; absolute risk reduction [ARR], 1.5%). For patients transported to level II trauma centers, helicopter transport was associated with an improved odds of survival (OR, 1.15; 95% CI, 1.13-1.17; P < .001; ARR, 1.4%). A greater proportion (18.2%) of those transported to level I trauma centers by helicopter were discharged to rehabilitation compared with 12.7% transported by ground services (P < .001), and 9.3% transported by helicopter were discharged to intermediate facilities compared with 6.5% by ground services (P < .001). Fewer patients transported by helicopter left level II trauma centers against medical advice (0.5% vs 1.0%, P < .001).
Conclusion Among patients with major trauma admitted to level I or level II trauma centers, transport by helicopter compared with ground services was associated with improved survival to hospital discharge after controlling for multiple known confounders.
A multidisciplinary panel of 28 experts from eight countries reviewed the literature and came up with consensus guidelines in point-of-care lung ultrasound. There were some big names involved – all the big players in emergency/critical care ultrasound from around the World. Conspicuously absent were Matt and Mike from the Emergency Ultrasound Podcast, but maybe there was a maximum awesomeness limit or something.
Here are some snippets, taken out of context and without the grade of recommendation attached. Try to get hold of the original if you can, which might not be easy. I never understand it when ‘international recommendations’ are published as subscription-only articles. Either they want people to follow them or not. Oh well – here are some of their recommendations: Pneumothorax
The sonographic signs of pneumothorax include the following: Presence of lung point(s); Absence of lung sliding; Absence of B-lines; Absence of lung pulse
The lung pulse refers to the subtle rhythmic movement of the visceral upon the parietal pleura with cardiac oscillations and is a rule-out sign for pneumothorax
In the supine patient, the sonographic technique consists of exploration of the least gravitationally dependent areas progressing more laterally.
Bedside lung ultrasound is a useful tool to differentiate between small and large pneumothorax, using detection of the lung point.
Interstitial syndrome
B-lines are defined as discrete laser-like vertical hyperechoic reverberation artifacts that arise from the pleural line (previously described as ‘‘comet tails’’), extend to the bottom of the screen without fading, and move synchronously with lung sliding.
The presence of multiple diffuse bilateral B-lines indicates interstitial syndrome. Causes of interstitial syndrome include the following conditions: Pulmonary edema of various causes; Interstitial pneumonia or pneumonitis; Diffuse parenchymal lung disease (pulmonary fibrosis)
Lung consolidation
The sonographic sign of lung consolidation is a subpleural echo-poor region or one with tissue-like echotexture.
Lung ultrasound is a clinically useful tool to rule in pneumonia; however, lung ultrasound does not rule out consolidations that do not reach the pleura.
In mechanically ventilated patients lung ultrasound should be considered as it is more accurate than portable chest radiography in the detection of consolidation.
Pleural effusion
Both of the following signs are present in almost all free effusions: A space (usually anechoic) between the parietal and visceral pleura; Respiratory movement of the lung within the effusion (‘‘sinusoid sign’’)
In opacities identified by chest radiography, lung ultrasound should be used because it is more accurate than chest radiography in distinguishing between effusion and consolidation.
Visualization of internal echoes, either of mobile particles or septa, is highly suggestive of exudate or hemothorax
BACKGROUND: The purpose of this study is to provide evidence-based and expert consensus recommendations for lung ultrasound with focus on emergency and critical care settings.
METHODS: A multidisciplinary panel of 28 experts from eight countries was involved. Literature was reviewed from January 1966 to June 2011. Consensus members searched multiple databases including Pubmed, Medline, OVID, Embase, and others. The process used to develop these evidence-based recommendations involved two phases: determining the level of quality of evidence and developing the recommendation. The quality of evidence is assessed by the grading of recommendation, assessment, development, and evaluation (GRADE) method. However, the GRADE system does not enforce a specific method on how the panel should reach decisions during the consensus process. Our methodology committee decided to utilize the RAND appropriateness method for panel judgment and decisions/consensus.
RESULTS: Seventy-three proposed statements were examined and discussed in three conferences held in Bologna, Pisa, and Rome. Each conference included two rounds of face-to-face modified Delphi technique. Anonymous panel voting followed each round. The panel did not reach an agreement and therefore did not adopt any recommendations for six statements. Weak/conditional recommendations were made for 2 statements, and strong recommendations were made for the remaining 65 statements. The statements were then recategorized and grouped to their current format. Internal and external peer-review processes took place before submission of the recommendations. Updates will occur at least every 4 years or whenever significant major changes in evidence appear.
CONCLUSIONS: This document reflects the overall results of the first consensus conference on “point-of-care” lung ultrasound. Statements were discussed and elaborated by experts who published the vast majority of papers on clinical use of lung ultrasound in the last 20 years. Recommendations were produced to guide implementation, development, and standardization of lung ultrasound in all relevant settings.