Primary percutaneous coronary intervention or fibrinolysis for STEMI? What if you don’t have PCI at your hospital?
The new 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction is out and you can get the summary here.
Here’s what they say about initial reperfusion therapy:
Onset of Myocardial Infarction: Recommendations
Regional Systems of STEMI Care, Reperfusion Therapy, and Time-to-Treatment Goals Class I
1. All communities should create and maintain a regional system of STEMI care that includes assessment and continuous quality improvement of emergency medical services and hospital-based activities. Performance can be facilitated by participating in programs such as Mission: Lifeline and the Door-to-Balloon Alliance.(Level of Evidence: B)
2. Performance of a 12-lead electrocardiogram (ECG) by emergency medical services personnel at the site of first medical contact (FMC) is recommended in patients with symptoms consistent with STEMI.(Level of Evidence: B)
3. Reperfusion therapy should be administered to all eligible patients with STEMI with symptom onset within the prior 12 hours. (Level of Evidence: A)
4. Primary PCI is the recommended method of reper- fusion when it can be performed in a timely fashion by experienced operators. (Level of Evidence: A)
5. Emergency medical services transport directly to a PCI-capable hospital for primary PCI is the recommended triage strategy for patients with STEMI, with an ideal FMC-to-device time system goal of 90 minutes or less.(Level of Evidence: B)
6. Immediate transfer to a PCI-capable hospital for primary PCI is the recommended triage strategy for patients with STEMI who initially arrive at or are transported to a non–PCI-capable hospital, with an FMC-to-device time system goal of 120 minutes or less.(Level of Evidence: B)
7. In the absence of contraindications, fibrinolytic therapy should be administered to patients with STEMI at non–PCI-capable hospitals when the anticipated FMC-to-device time at a PCI-capable hospital exceeds 120 minutes because of unavoidable delays.(Level of Evidence: B)
8. When fibrinolytic therapy is indicated or chosen as the primary reperfusion strategy, it should be administered within 30 minutes of hospital arrival.(Level of Evidence: B) Class IIa
1. Reperfusion therapy is reasonable for patients with STEMI and symptom onset within the prior 12 to 24 hours who have clinical and/or ECG evidence of ongoing ischemia. Primary PCI is the preferred strategy in this population. (Level of Evidence: B)
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2012 Dec 17. [Epub ahead of print]
Nonoperative management of blunt hepatic injuries currently is the treatment modality of choice in hemodynamically stable patients, irrespective of the grade of injury or patient age.
Patients presenting with hemodynamic instability and peritonitis still warrant emergent operative intervention.
Intravenous contrast enhanced computed tomographic scan is the diagnostic modality of choice for evaluating blunt hepatic injuries.
Selective nonoperative management of blunt splenic injury
Nonoperative management of blunt splenic injuries is now the treatment modality of choice in hemodynamically stable patients, irrespective of the grade of injury, patient age, or the presence of associated injuries.
Patients presenting with hemodynamic instability and peritonitis still warrant emergent operative intervention.
Intravenous contrast enhanced computed tomographic scan is the diagnostic modality of choice for evaluating blunt splenic injuries.
Screening for blunt cardiac injury
Electrocardiogram (ECG) alone is not sufficient to rule out BCI.
BCI can be ruled out only if both ECG result and troponin I level are normal, a significant change from the previous guideline.
Patients with new ECG changes and/or elevated troponin I should be admitted for monitoring.
Echocardiogram is not beneficial as a screening tool for BCI and should be reserved for patients with hypotension and/or arrhythmias.
The presence of a sternal fracture alone does not predict BCI.
Cardiac computed tomography or magnetic resonance imaging can be used to differentiate acute myocardial infarction from BCI in trauma patients.
Evaluation and management of penetrating lower extremity arterial trauma
Expedited triage of patients is possible with physical examination and/or the measurement of ankle-brachial indices.
Computed tomographic angiography has become the diagnostic study of choice when imaging is required.
Tourniquets and intravascular shunts have emerged as adjuncts in the treatment of penetrating lower extremity arterial trauma.
Prophylactic antibiotic use in penetrating abdominal trauma
There is evidence to support a Level I recommendation that prophylactic antibiotics should only be administered for 24 hours in the presence of a hollow viscus injury.
There are no data to support continuing prophylactic antibiotics longer than 24 hours in damage control laparotomy.
Screening for thoracolumbar spinal injuries in blunt trauma
Multidetector computed tomographic scans have become the screening modality of choice and the criterion standard in screening for TLS injuries.
Patients without altered mentation or significant mechanism may be excluded by clinical examination without imaging.
Patients with gross neurologic deficits or concerning clinical examination findings with negative imaging should receive a magnetic resonance imaging expediently, and the spine service should be consulted
Emergency tracheal intubation immediately following traumatic injury
The decision to intubate a patient following traumatic injury is based on multiple factors, including the need for oxygenation and ventilation, the extent and mechanism of injury, predicted operative need, or progression of disease.
Rapid sequence intubation with direct laryngoscopy continues to be the recommended method for ETI, although the use of airway adjuncts such as blind insertion supraglottic devices and video laryngoscopy may be useful in facilitating successful ETI and may be preferred in certain patient populations.
There is no pharmacologic induction agent of choice for ETI; however, succinylcholine is the neuromuscular blockade agent recommended for rapid sequence intubation.
Presumptive antibiotic use in tube thoracostomy for traumatic hemopneumothorax
Routine presumptive antibiotic use to reduce the incidence of empyema and pneumonia in TT for traumatic hemopneumothorax is controversial; however, there is insufficient published evidence to support any recommendation either for or against this practice.
Evaluation and management of geriatric trauma
Effective evidence-based care of aging patients necessitates aggressive triage, correction of coagulopathy, and limitation of care when clinical evidence points toward an overwhelming likelihood of poor long-term prognosis
Management of pulmonary contusion and flail chest
Patients with PC-FC should not be excessively fluid restricted but should be resuscitated to maintain signs of adequate tissue perfusion.
Obligatory mechanical ventilation in the absence of respiratory failure should be avoided.
The use of optimal analgesia and aggressive chest physiotherapy should be applied to minimize the likelihood of respiratory failure.
Epidural catheter is the preferred mode of analgesia delivery in severe flail chest injury.
Paravertebral analgesia may be equivalent to epidural analgesia and may be appropriate in certain situations when epidural is contraindicated.
A trial of mask continuous positive airway pressure should be considered in alert patients with marginal respiratory status.
Patients requiring mechanical ventilation should be supported in a manner based on institutional and physician preference and separated from the ventilator at the earliest possible time.
Positive end-expiratory pressure or continuous positive airway pressure should be provided.
High-frequency oscillatory ventilation should be considered for patients failing conventional ventilatory modes. Independent lung ventilation may also be considered in severe unilateral pulmonary contusion when shunt cannot be otherwise corrected.
Surgical fixation of flail chest may be considered in cases of severe flail chest failing to wean from the ventilator or when thoracotomy is required for other reasons.
Self-activating multidisciplinary protocols for the treatment of chest wall injuries may improve outcome and should be considered where feasible.
Steroids should not be used in the therapy of pulmonary contusion.
Diuretics may be used in the setting of hydrostatic fluid overload in hemodynamically stable patients or in the setting of known concurrent congestive heart failure.
Evaluation and management of small-bowel obstruction
Level I evidence now exists to recommend the use of computed tomographic scan, especially multidetector computed tomography with multiplanar reconstructions, in the evaluation of patients with SBO because it can provide incremental clinically relevant information over plains films that may lead to changes in management.
Patients with evidence of generalized peritonitis, other evidence of clinical deterioration, such as fever, leukocytosis, tachycardia, metabolic acidosis, and continuous pain, or patients with evidence of ischemia on imaging should undergo timely exploration.
The remainder of patients can safely undergo initial nonoperative management for both partial and complete SBO.
Water-soluble contrast studies should be considered in patients who do not clinically resolve after 48 to 72 hours for both diagnostic and potential therapeutic purposes.
Laparoscopic treatment of SBO has been demonstrated to be a viable alternative to laparotomy in selected cases.
The UK’s National Institute for Health and Clinical Excellence has issued updated guidance on the management of acute upper gastrointestinal bleeding.
The initial resuscitation section recommends haemostatic blood product resuscitation for unstable patients in line with massive transfusion practice in trauma.
A risk assessment is recommended using the Blatchford score pre-endoscopy at first assessment, and the full Rockall score after endoscopy.
Consider early discharge for patients with a pre-endoscopy Blatchford score of 0.
In non-varicesal haemorrhage, acid-suppression drugs (proton pump inhibitors or H2-receptor antagonists) before endoscopy are not recommended.
Terlipressin should be given to patients with suspected variceal bleeding at presentation and continued until definitive haemostasis has been achieved, or after 5 days, unless there is another indication for its use.
Prophylactic antibiotic therapy should be offered at presentation to patients with suspected or confirmed variceal bleeding.
Click image to go to interactive pathway on NICE website
A study of nonshockable out of hospital cardiac arrest survival showed significant improvement in short- and long-term survival and neurological outcome after implementation of a protocol consistent with CPR guidelines that prioritised chest compressions. These improvements were especially evident among arrests attributable to a cardiac cause, although there was no evidence of harm among arrests attributable to a noncardiac cause.
This was not a randomised trial so unrecognised factors may have contributed to the improved outcome in addition to the change in CPR protocol. However, it is interesting as it provides up to date survival rates from a large population sample: Non shockable out of hospital cardiac arrests achieve return of spontaneous circulation in 34%, 6.8% are discharged from hospital (5.1% with a favourable neurological outcome), and 4.9% survived one year.
The breakdown between PEA and asystole is of course telling, and unsurprising, with 12.8% versus 1.1% being discharged with a favourable neurological outcome, respectively. I would imagine then that some of the PEA patients had beating hearts with hypotension extreme enough to cause pulselessness (pseudo-electromechanical dissociation) – clinically a ‘cardiac arrest’ but really nothing of the sort, and the reason we use cardiac ultrasound to prognosticate.
BACKGROUND: Out-of-hospital cardiac arrest (OHCA) claims millions of lives worldwide each year. OHCA survival from shockable arrhythmias (ventricular fibrillation/ tachycardia) improved in several communities after implementation of American Heart Association resuscitation guidelines that eliminated “stacked” shocks and emphasized chest compressions. “Nonshockable” rhythms are now the predominant presentation of OHCA; the benefit of such treatments on nonshockable rhythms is uncertain.
METHODS AND RESULTS: We studied 3960 patients with nontraumatic OHCA from nonshockable initial rhythms treated by prehospital providers in King County, Washington, over a 10-year period. Outcomes during a 5-year intervention period after adoption of new resuscitation guidelines were compared with the previous 5-year historical control period. The primary outcome was 1-year survival. Patient demographics and resuscitation characteristics were similar between the control (n=1774) and intervention (n=2186) groups, among whom 471 of 1774 patients (27%) versus 742 of 2186 patients (34%), respectively, achieved return of spontaneous circulation; 82 (4.6%) versus 149 (6.8%) were discharged from hospital, 60 (3.4%) versus 112 (5.1%) with favorable neurological outcome; 73 (4.1%) versus 135 (6.2%) survived 1 month; and 48 (2.7%) versus 106 patients (4.9%) survived 1 year (all P≤0.005). After adjustment for potential confounders, the intervention period was associated with an improved odds of 1.50 (95% confidence interval, 1.29-1.74) for return of spontaneous circulation, 1.53 (95% confidence interval, 1.14-2.05) for hospital survival, 1.56 (95% confidence interval, 1.11-2.18) for favorable neurological status, 1.54 (95% confidence interval, 1.14-2.10) for 1-month survival, and 1.85 (95% confidence interval, 1.29-2.66) for 1-year survival.
CONCLUSION: Outcomes from OHCA resulting from nonshockable rhythms, although poor by comparison with shockable rhythm presentations, improved significantly after implementation of resuscitation guideline changes, suggesting their potential to benefit all presentations of OHCA.
Impact of changes in resuscitation practice on survival and neurological outcome after out-of-hospital cardiac arrest resulting from nonshockable arrhythmia Circulation. 2012 Apr 10;125(14):1787-94
A case is reported in Prehospital Emergency Care1 in which an agitated patient (due to mania and alcohol intoxication) received 5 mg/kg (500 mg) of ketamine intramuscularly by an EMS crew which dissociated him within a few minutes. He subsequently developed episodes of laryngospasm in the emergency department which were unrelieved by head tilt, chin lift and simple airway adjuncts but responded to bag-mask ventilation (BMV). The patient was intubated because the laryngospasm recurred, although it had again responded to BMV.
The authors make the point that because of the response of laryngospasm to simple manoeuvres, and because in the prehospital environment a patient will not be left without an EMS provider present, ‘restricting ketamine to EMS units capable of rapid-sequence intubation therefore seems unnecessary.‘
This is one for EMS directors to consider seriously. Personally, I think practicing prehospital care without access to ketamine is like having a hand tied behind my back. Ketamine opens up a world of possibilities in controlling combative patients, optimising scene safety, providing sedation for painful procedures including extrication, and enabling severe pain to be controlled definitively.
I’ve been using ketamine regularly for prehospital analgesia and emergency department procedural sedation in both adults and kids for more than a decade. I’ve seen significant laryngospasm 5 times (twice in kids). On one of those occasions, a 3 year old child desaturated to around 50% twice during two episodes of laryngospasm. We weren’t slow to pick it up – that was just her showing us how quickly kids can desaturate which continued while we went through a stepwise approach until BMV resolved it. It was however an eye opener for the registrar (senior resident) assisting me, who became extremely respectful of ketamine after that. Our ED sedation policy (that I wrote) required that suxamethonium was ready and available and that an appropriate dose had been calculated before anyone got ketamine. Paralysis may extremely rarely be required, but when it’s needed you need to be ready.
The best monitor for laryngospasm – noninvasive capnography
Laryngospasm is rare but most regular prescribers of ketamine will have seen it; the literature says it occurs in about 1-2% of sedations, although anecdotally I think it’s a bit less frequent. Importantly for those weighing the risks of allowing non-RSI competent prescribers, the requirement for intubation is exceptionally rare (2 of 11,589 reported cases in one review). Anyone interested should read this excellent review of ketamine-related adverse effects provided by Chris Nickson at Life in The Fast Lane. Chris reminds us of the Larson manouevre, which is digital pressure in the notch behind and below the ear, described by Larson2 as follows:
The technique involves placing the middle finger of each hand in what I term the laryngospasm notch. This notch is behind the lobule of the pinna of each ear. It is bounded anteriorly by the ascending ramus of the mandible adjacent to the condyle, posteriorly by the mastoid process of the temporal bone, and cephalad by the base of the skull. The therapist presses very firmly inward toward the base of the skull with both fingers, while at the same time lifting the mandible at a right angle to the plane of the body (i.e., forward displacement of the mandible or “jaw thrust”). Properly performed, it will convert laryngospasm within one or two breaths to laryngeal stridor and in another few breaths to unobstructed respirations.
I use this point most often to provide painful stimuli when assessing GCS in a patient, particular those I think may be feigning unconsciousness (I’ve done this for a number of years since learning how painful it can be when I was shown it by a jujitsu instructor). Dr Larson says he was taught the technique by Dr Guadagni, so perhaps we should be calling it the ‘Guadagni manouevre’. The lack of published evidence has led to some appropriate skepticism3, but as it can be combined with a jaw thrust it needn’t delay more aggressive interventions should they become necessary, it may work, and it’s likely to be harmless.
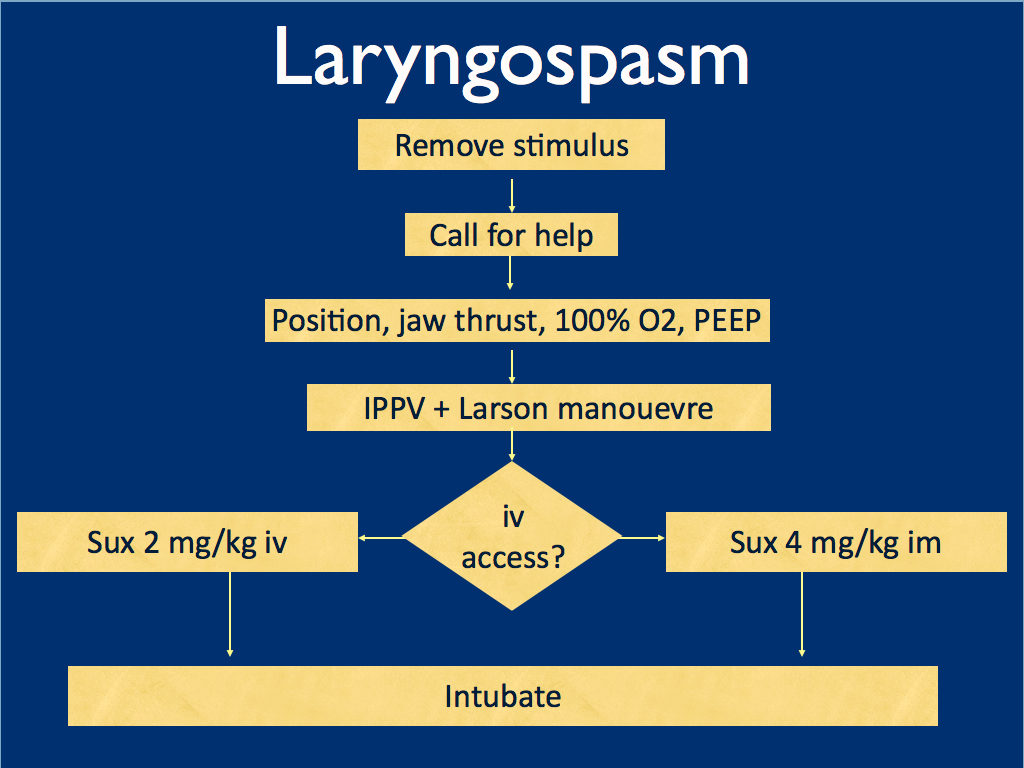
I presented the following suggested algorithm for management of laryngospasm during ketamine procedural sedation at a regional emergency medicine ‘Fellows Forum’ meeting in November 2007 in the UK. Since many paediatric procedural sedations were done using intramuscular (im) ketamine, it gives guidance based on whether or not vascular access has been obtained:
Some things I considered were:
Neuromuscular blockade (NMB) isn’t always necessary – laryngospasm may be managed with other sedatives such as propofol. However, titrating further sedatives in a desaturating child in my view is inferior to definitive airway management and laryngeal relaxation with suxamethonium and a tube.
Laryngospasm may be managed with much smaller doses of suxamethonium than are required for intubation – as little as 0.1 mg/kg may be effective. However, I think once we go down the NMB route we’re committed to intubation and therefore we should use a dose guaranteed to be effective in achieving intubating conditions.
In the child without vascular access, I considered intraosseous and intralingual sux. However, intramuscular suxamethonium is likely to have a relaxant effect on the laryngeal muscles within 30-45 seconds, which has to be compared with time taken to insert and confirm intraosseous needle placement. I do not think the traditionally recommended intralingual injection has any role to play in modern airway management.
At the time I wrote this most paediatric resuscitation bays in my area in the United Kingdom had breathing circuits capable of delivering PEEP – usually the Ayr’s T-Piece (specifically the Mapleson F system), which is why PEEP was included early in in the algorithm prior to BMV.
I have since modified it for two reasons: firstly, we might as well do the Larson manoeuvre during the jaw thrust; secondly, many Australasian and US EDs will only be able to deliver PEEP with a PEEP valve attached to a BVM, so PEEP has been moved to the BVM stage.
I would love to hear what people are doing in their prehospital and inhospital practice. Should ketamine only be administered by providers who can offer RSI? Do you have a laryngospasm protocol? If so, I’d love to see it. If not, feel free to use or adapt my unvalidated one at your own risk.
ABSTRACT An advanced life support emergency medical services (EMS) unit was dispatched with law enforcement to a report of a male patient with a possible overdose and psychiatric emergency. Police restrained the patient and cleared EMS into the scene. The patient was identified as having excited delirium, and ketamine was administered intramuscularly. Sedation was achieved and the patient was transported to the closest hospital. While in the emergency department, the patient developed laryngospasm and hypoxia. The airway obstruction was overcome with bag–valve–mask ventilation. Several minutes later, a second episode of laryngospasm occurred, which again responded to positive-pressure ventilation. At this point the airway was secured with an endotracheal tube. The patient was uneventfully extubated several hours later. This is the first report of laryngospam and hypoxia associated with prehospital administration of intramuscular ketamine to a patient with excited delirium.
Some defibrillators have accelerometers capable of measuring chest compression depth during CPR. This allowed a study correlating compression depth with survival in out of hospital cardiac arrest.
More than half of patients received less than the 2005 recommended chest compression depth of 38–51 mm and >90% received less than the 2010 recommended depth of >50 mm. There was an inverse relationship between rate and depth, ie. rescuers had a tendency to ‘push hard, push slow’ or ‘push soft, push fast’.
The authors state: We found an association between adequate compression depth and good outcomes but could not demonstrate that the 2010 recommendations are better than those from 2005. Although we believe that compression depth is an important component of CPR and should be measured routinely during cardiac arrest resuscitation, we believe that the optimal depth is currently unknown.
BACKGROUND: The 2010 international guidelines for cardiopulmonary resuscitation recently recommended an increase in the minimum compression depth from 38 to 50 mm, although there are limited human data to support this. We sought to study patterns of cardiopulmonary resuscitation compression depth and their associations with patient outcomes in out-of-hospital cardiac arrest cases treated by the 2005 guideline standards.
DESIGN: Prospective cohort.
SETTING: Seven U.S. and Canadian urban regions.
PATIENTS: We studied emergency medical services treated out-of-hospital cardiac arrest patients from the Resuscitation Outcomes Consortium Epistry-Cardiac Arrest for whom electronic cardiopulmonary resuscitation compression depth data were available, from May 2006 to June 2009.
MEASUREMENTS: We calculated anterior chest wall depression in millimeters and the period of active cardiopulmonary resuscitation (chest compression fraction) for each minute of cardiopulmonary resuscitation. We controlled for covariates including compression rate and calculated adjusted odds ratios for any return of spontaneous circulation, 1-day survival, and hospital discharge.
MAIN RESULTS: We included 1029 adult patients from seven U.S. and Canadian cities with the following characteristics: Mean age 68 yrs; male 62%; bystander witnessed 40%; bystander cardiopulmonary resuscitation 37%; initial rhythms: Ventricular fibrillation/ventricular tachycardia 24%, pulseless electrical activity 16%, asystole 48%, other nonshockable 12%; outcomes: Return of spontaneous circulation 26%, 1-day survival 18%, discharge 5%. For all patients, median compression rate was 106 per minute, median compression fraction 0.65, and median compression depth 37.3 mm with 52.8% of cases having depth <38 mm and 91.6% having depth <50 mm. We found an inverse association between depth and compression rate ( p < .001). Adjusted odds ratios for all depth measures (mean values, categories, and range) showed strong trends toward better outcomes with increased depth for all three survival measures.
CONCLUSIONS: We found suboptimal compression depth in half of patients by 2005 guideline standards and almost all by 2010 standards as well as an inverse association between compression depth and rate. We found a strong association between survival outcomes and increased compression depth but no clear evidence to support or refute the 2010 recommendations of >50 mm. Although compression depth is an important component of cardiopulmonary resuscitation and should be measured routinely, the most effective depth is currently unknown.
The AABB (formerly the American Association of Blood Banks has issued guidelines on red blood cell transfusion1, providing some number-based targets which may be helpful for some practitioners or organisations. Editorialist and heavyweight intensivist Jean-Louis Vincent argues for a more individual patient-based assessment2, and highlights some of the weaknesses of existing studies, in particular the often quoted but now fairly old TRICC study3 which suffered from poor recruitment and the possible lack of applicability to modern practice now that leucodepleted products are used.
Prof Vincent states:
“Transfusion decisions need to consider individual patient characteristics, including age and the presence of CAD, to estimate a specific patient’s likelihood of benefit from transfusion. The decision to transfuse is too complex and important to be guided by a single number.”
Description: Although approximately 85 million units of red blood cells (RBCs) are transfused annually worldwide, transfusion practices vary widely. The AABB (formerly, the American Association of Blood Banks) developed this guideline to provide clinical recommendations about hemoglobin concentration thresholds and other clinical variables that trigger RBC transfusions in hemodynamically stable adults and children.
Methods: These guidelines are based on a systematic review of the literature on randomized clinical trials evaluating transfusion thresholds. We performed a literature search from 1950 to February 2011 with no language restrictions. We examined the proportion of patients who received any RBC transfusion and the number of RBC units transfused to describe the effect of restrictive transfusion strategies on RBC use. To determine the clinical consequences of restrictive transfusion strategies, we examined overall mortality, nonfatal myocardial infarction, cardiac events, pulmonary edema, stroke, thromboembolism, renal failure, infection, hemorrhage, mental confusion, functional recovery, and length of hospital stay.
Recommendation 1: The AABB recommends adhering to a restrictive transfusion strategy (7 to 8 g/dL) in hospitalized, stable patients (Grade: strong recommendation; high-quality evidence).
Recommendation 2: The AABB suggests adhering to a restrictive strategy in hospitalized patients with preexisting cardiovascular disease and considering transfusion for patients with symptoms or a hemoglobin level of 8 g/dL or less (Grade: weak recommendation; moderate-quality evidence).
Recommendation 3: The AABB cannot recommend for or against a liberal or restrictive transfusion threshold for hospitalized, hemodynamically stable patients with the acute coronary syndrome (Grade: uncertain recommendation; very low-quality evidence).
Recommendation 4: The AABB suggests that transfusion decisions be influenced by symptoms as well as hemoglobin concentration (Grade: weak recommendation; low-quality evidence).
‘You can’t clear the cervical spine until the patient wakes up!’ How often have you heard this said about a patient with severe traumatic brain injury who may not ‘wake up’ for weeks, if at all?
A controversial area, but many institutions now allow collar removal if a neck CT scan is normal. Does this rule out injury with 100% sensitivity? No – but it probably pushes the balance of risk towards removing the collar – an intervention with no evidence for benefit and plenty of reasons why it may be harmful to ventilated ICU patients. For example, clearing the cervical spine based on MDCT was associated with less delirium and less ventilator associated pneumonia, both of which have been associated with increased mortality in critically ill patients (this is referenced in the paper below).
The UK’s Intensive Care Society has had pragmatic guidelines along these lines since 2005, which can be found here. This month’s Intensive Care Medicine publishes an updated literature review providing some further support to this approach.
PURPOSE: Controversy exists over how to ‘clear’ (we mean enable the clinician to safely remove spinal precautions based on imaging and/or clinical examination) the spine of significant unstable injury among clinically unevaluable obtunded blunt trauma patients (OBTPs). This review provides a clinically relevant update of the available evidence since our last review and practice recommendations in 2004.
METHODS: Medline, Embase. Google Scholar, BestBETs, the trip database, BMJ clinical evidence and the Cochrane library were searched. Bibliographies of relevant studies were reviewed.
RESULTS: Plain radiography has low sensitivity for detecting unstable spinal injuries in OBTPs whereas multidetector-row computerised tomography (MDCT) approaches 100%. Magnetic resonance imaging (MRI) is inferior to MDCT for detecting bony injury but superior for detecting soft tissue injury with a sensitivity approaching 100%, although 40% of such injuries may be stable and ‘false positive’. For studies comparing MDCT with MRI for OBTPs; MRI following ‘normal’ CT may detect up to 7.5% missed injuries with an operative fixation in 0.29% and prolonged collar application in 4.3%. Increasing data is available on the complications associated with prolonged spinal immobilisation among a population where a minority have an actual injury.
CONCLUSIONS: Given the variability of screening performance it remains acceptable for clinicians to clear the spine of OBTPs using MDCT alone or MDCT followed by MRI, with implications to either approach. Ongoing research is needed and suggestions are made regarding this. It is essential clinicians and institutions audit their data to determine their likely screening performances in practice.
The prevention and management of venous thromboembolic disease is a huge topic, which generates questions for emergency, critical care, and acute physicians during many shifts:
How long should someone requiring cardioversion for atrial fibrillation be anticoagulated for?
How should I provide thromboprophylaxis for this intubated patient?
This patient with submassive pulmonary embolism isn’t hypotensive yet. Can I thrombolyse them? Can I?
There’s a large superficial vein thrombosis in that limb – is anticoagulation indicated?
This asymptomatic patient on warfarin has an INR of 9.0 – should I reverse them?
Do I need to add Vitamin K if I’ve reversed warfarin with prothrombin complex concentrate?
The answers to these – and many, many more – questions are provided in one of the most comprehensive guidelines I’ve ever come across. I can see myself clicking on the link below in future when on duty in the ED. Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines Chest. 2012 Feb;141(2 Suppl) Full Text
The European Society of Intensive Care Medicine has produced a consensus statement on colloid volume therapy for critically ill patients, published in this month’s Intensive Care Medicine.
Curiously, the full text document is not yet availablle on ESICM’s website, but I found this presentation summarising the work by one the authors (Richard Beale):
PURPOSE: Colloids are administered to more patients than crystalloids, although recent evidence suggests that colloids may possibly be harmful in some patients. The European Society of Intensive Care Medicine therefore assembled a task force to compile consensus recommendations based on the current best evidence for the safety and efficacy of the currently most frequently used colloids-hydroxyethyl starches (HES), gelatins and human albumin.
METHODS: Meta-analyses, systematic reviews and clinical studies of colloid use were evaluated for the treatment of volume depletion in mixed intensive care unit (ICU), cardiac surgery, head injury, sepsis and organ donor patients. Clinical endpoints included mortality, kidney function and bleeding. The relevance of concentration and dosage was also assessed. Publications from 1960 until May 2011 were included. The quality of available evidence and strength of recommendations were based on the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach.
RECOMMENDATIONS AND CONCLUSIONS: We recommend not to use HES with molecular weight ≥200 kDa and/or degree of substitution >0.4 in patients with severe sepsis or risk of acute kidney injury and suggest not to use 6% HES 130/0.4 or gelatin in these populations. We recommend not to use colloids in patients with head injury and not to administer gelatins and HES in organ donors. We suggest not to use hyperoncotic solutions for fluid resuscitation. We conclude and recommend that any new colloid should be introduced into clinical practice only after its patient-important safety parameters are established.
Consensus statement of the ESICM task force on colloid volume therapy in critically ill patients Intensive Care Med. 2012 Mar;38(3):368-83 Update September 2012:
An RCT showed patients with severe sepsis assigned to fluid resuscitation with HES 130/0.42 had an increased risk of death at day 90 and were more likely to require renal-replacement therapy, as compared with those receiving Ringer’s acetate. Read more about the trial here Hydroxyethyl Starch 130/0.42 versus Ringer’s Acetate in Severe Sepsis N Engl J Med. 2012 Jul 12;367(2):124-34
Australian intensivist John Myburgh gives a great summary of Fluid Therapy in critical care here