This video shows the mechanism for dislodgement and deformation of humeral intraosseous needles and how to avoid this.
In summary, if you need to abduct the arm (eg. for thoracostomy), keep the thumbs down (ie. have the arm internally rotated at the shoulder). Otherwise the IO catheter may bend or fall out.
Occasionally we step out of the resuscitation room feeling like a case should have gone better, but it can be hard to put our finger on just where it went wrong. In my last post I discussed the STEPS approach to analysing resuscitation cases: Self, Team, Environment, Patient and System.
Occasionally you can get a case where the STEPS seem to be aligned but things still feel bad. In which the outcome was unsatisfactory because the plan was wrong, or the team wasn’t able to execute the plan. Consider the following case.
1. A patient with a past history of DVT no longer on anticoagulants presents with chest pain and syncope.
She is severely hypotensive with a raised jugular venous pressure and a clear chest x-ray. A working diagnosis of pulmomary embolism is made.
Discussions ensue regarding empirical fibrinolysis and a respiratory physician is consulted, who over the phone cautions against treating without a CT pulmonary angiogram.
The patient is given heparin and transferred to the CT scanner where she arrests. Intravenous rtPA is given during CPR but no return of spontaneous circulation is achieved and she is pronounced dead after 30 minutes of resuscitation.
On this occasion the team worked efficiently and communicated well under clear leadership. Everyone knew the plan and shared the mental model. The environment was well controlled and the patient had been swiftly moved to CT within 20 minutes of arrival. Thanks to simulation training the well rehearsed cardiac arrest resuscitation was conducted with precision and the team was able to rapidly access the thrombolytic and knew the correct dose.
By a quick STEPS analysis, this case appears to have gone as well as could be expected. Perhaps there is nothing to learn. Some you win, some you lose, no?
No. Autopsy revealed type A aortic dissection with pericardial tamponade.
The management may have been efficient but it failed to be effective. In other words, things were done right, but the right things weren’t done; they did the wrong things right.
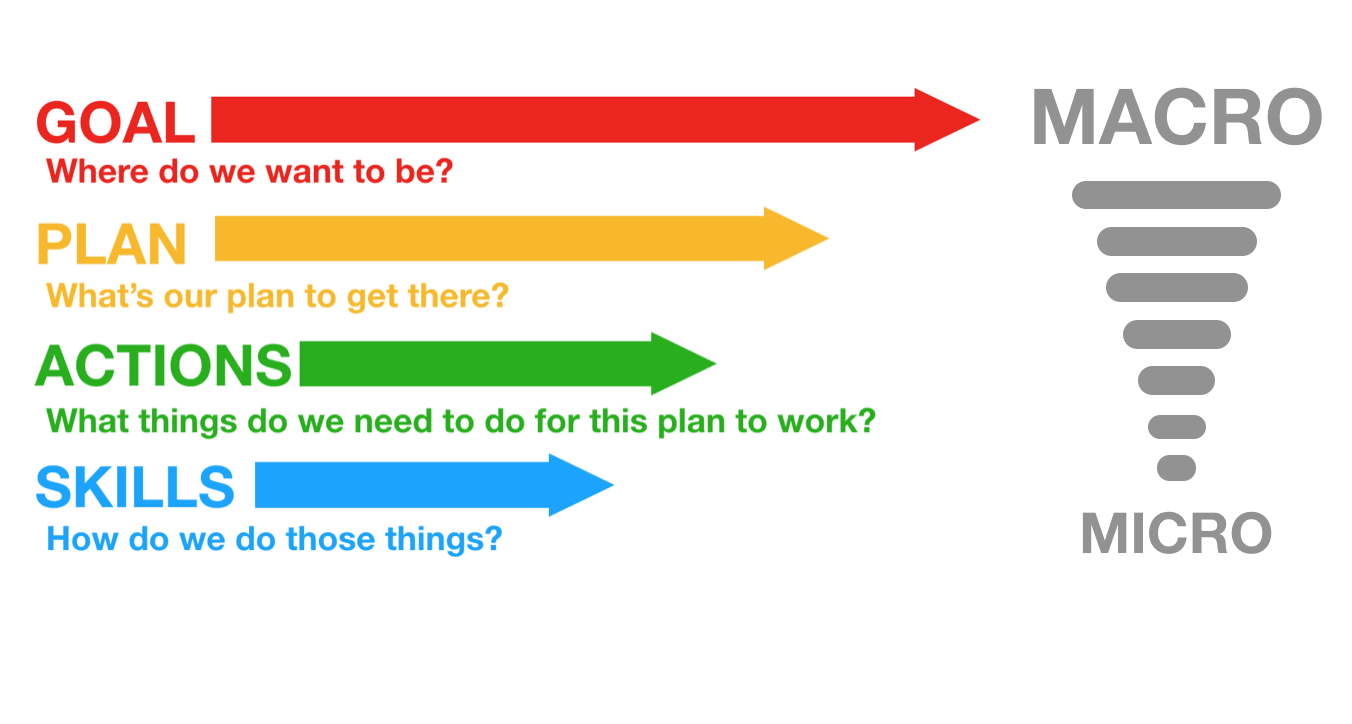
This might be an example where STEPS is inadequate, and instead we should evaluate the clinical trajectory. The cognitive bias that led to a lack of consideration of alternative diagnoses might be classifiable under ‘self’ or ‘team’ but I find it more helpful to consider it under a failure of strategy. What is strategy? Strategy in my mind is another word for plan. The plan is based on a particular resuscitation goal, and will consist of the procedures & skills required to action the plan. We can thus break down an attempted clinical trajectory into:
Goal (what are we trying to achieve) Strategy, or Plan (what’s our plan to get there?) Tactics, or Actions (what procedures will be required to execute the plan) And, at more granular level: If we’re failing at the procedural level, the components of procedures, namely Skills & Microskills. So, as we zoom in from macro to micro in setting the clinical trajectory, we can look at Goals, Plan, Actions, and Skills: In the above case it appears the following was applied, in terms of Goal-Plan-Actions-Skills:
G – resuscitate hypotensive patient P – give fibrinolysis for likely PE A – consult respiratory physician, get CTPA S – request scan, give heparin, transport to CT
The goal was appropriate, but the plan was ineffective.
The following approach would have been more effective.
G – resuscitate hypotensive patient P – identify cause of undifferentiated hypotension and initiate treatment in the resus room A – thorough bedside assessment in patient too sick to move: history, physical, CXR, ECG, labs, POCUS S – Basic cardiac ultrasound
By planning to identify and treat the cause of hypotension in the resus room, the more appropriate investigation would have been selected (cardiac ultrasound) and the correct diagnosis is much more likely to have been made.
Let’s look at some other cases:
2. An 88-year-old male presents by ambulance to the ED with dizziness. He is hypotensive, pyrexial, hypoxic and confused.
His chest x-ray shows likely bronchopneumonia. He has appropriate initial resuscitation and ICU is consulted. Soon he is intubated and on high dose vasoactive medication with escalating doses despite ongoing hypotension, anuria, and a lactate of 11 mmol/l, increased from 8 on arrival.
As he is being wheeled off down the corridor towards ICU his distraught and frail wife arrives. She is taken to the quiet room where she explains that her husband would never want to be ‘on a life support machine’ and asks ‘can’t you just keep him comfortable’?
G – the goal – to provide maximally aggressive resuscitation – was not in keeping with the patient’s wishes. If the goal had been to provide care in accordance with his wishes, the plan could have included attempts to ascertain these sooner while providing initial treatment. Upon gaining sufficient information, a new goal can be established: maximising the patient’s comfort and dignity.
3. An obese 30-year-old female presents with syncope. At triage she is pale, tachycardic & hypotensive. Clinical and sonographic assessment, including free intraperitoneal fluid and a positive urine HCG, is suggestive of ruptured ectopic pregnancy.
The gynaecologist and anaesthetist ask the ED team to bring the patient straight to the operating room. The ED team spends 20 minutes struggling to obtain intravenous access, eventually placing a 22G intravenous catheter in the patient’s hand and a humeral intraosseous needle.
Her shock is considerably worse on arrival in theatre, despite attempts to transfuse O negative blood en route.
Goal – get her safely to the operating room Plan – vascular access, cross match blood, start haemostatic resuscitation, go to OR as soon as possible Actions – peripheral and/or intraosseous cannulation attempts Skills – vascular access skills
Here the failure was at the actions and skills level. Better vascular access could have been attained using ultrasound guided peripheral cannulation, or central vascular access, or earlier intraosseous insertion.
4. A 120kg 32-year-old male with a history of deliberate self harm presents on the night shift with coma due to mixed benzodiazepine and venlafaxine overdose.
The decision is made to intubate for airway protection. After rapid sequence induction direct laryngoscopy is attempted by the emergency registrar who obtains a grade 4 view. Cricoid pressure is removed resulting in a grade 3 view.
The registrar asks for a bougie which she passes and then railroads the tracheal tube over it. The cuff is inflated, capnography is connected, and the self-inflating bag is connected and squeezed while the chest is auscultated.
The abdomen distends, the capnograph remains flat, and gastric contents are seen to pass upward through the tube into the self-inflating bag. The tube is immediately removed and bag-mask ventilation is attempted. The oxygen saturation is now 78% and the airway is soiled. The airway is suctioned and repeat attempts to bag-mask ventilate fail. A successful cricothyroidotomy is performed and the patient subsequent has full neurological recovery.
Goal – Provide supportive care and minimise complications from overdose Plan – Airway protection and admit to ICU for monitoring Actions – Rapid sequence intubation, ICU referral Skills – Pre-, peri- and post-intubation oxygenation techniques; patient positioning; rapid sequence induction of anaesthesia; direct laryngoscopy; bougie handling techniques; external laryngeal manipulation
In this case the patient was not placed in the ramped position and no nasal cannulae were applied for apnoeic oxygenation. A tube was railroaded over an oesophageal bougie, which arguably should not occur if ‘hold up’ is sought when the bougie is placed.
Although the goal, plan and actions were appropriate, the team did not demonstrate adequate skill in this procedure. Likely due to a failure of training, standardised procedures, and checklists (or their application), this could also be identified as a ‘system’ problem in STEPS. It is also possible that the intubator forgot her training under stress – a problem classifiable under ‘self’. Alternatively other members of the team may have had knowledge but didn’t speak up or cross-check their colleague, which would be a ‘team’ issue.
Limitations of this approach This sort of analysis is retrospective and subjective and at risk of hindsight bias (e.g. distortion due to projection, denial, or selective recall). However, these limitations do not negate the value of the learning exercise, particularly if we are aware of them and strive to minimise their impact (e.g. write down the details of a cases as soon as possible afterward). It at least provides a structure for individuals and teams to begin the conversation about where and how things may have been suboptimal.
Goals may be multiple and may change according to incoming information, and for each goal there may be several viable alternative plans. STEPS and GPAS may overlap, eg. team failures may result in inappropriate goals and strategies, or in failed procedures.
Summary These models may prove helpful as a means of dissecting a case in a structured way. Put simply, STEPS offers a structure for identifying efficiency improvements (“doing things right”) and GPAS can help us assess effectiveness (“doing the right things”).
Another way of looking at it is that STEPS provides the components of a resus at any point in time, and GPAS defines the trajectory: where the resus is going and how to get there.
I use this structure to analyse cases in my own clinical practice and in my teaching. I would be interested to hear from others’ experience. Do you find this approach useful in identifying areas for improvement in those cases that you feel should have gone better?
Thanks to Chris Nickson for his comments and improvements to this post
A resuscitationist agonises. These words, expressed by Scott Weingart during a podcast we did together, ring true to all of us who strive to improve our practice. Driven by the passionate conviction that we should never lose a salvageable patient through imperfect care, we relive cases and re-run them through our mental simulators to identify areas for improvement.
In the search for actionable items though, we occasionally exit this process empty-handed. Something about a case felt wrong although ostensibly all the clinical interventions may have been appropriate. It is in these cases that it can be helpful to have a structure to aid analysis.
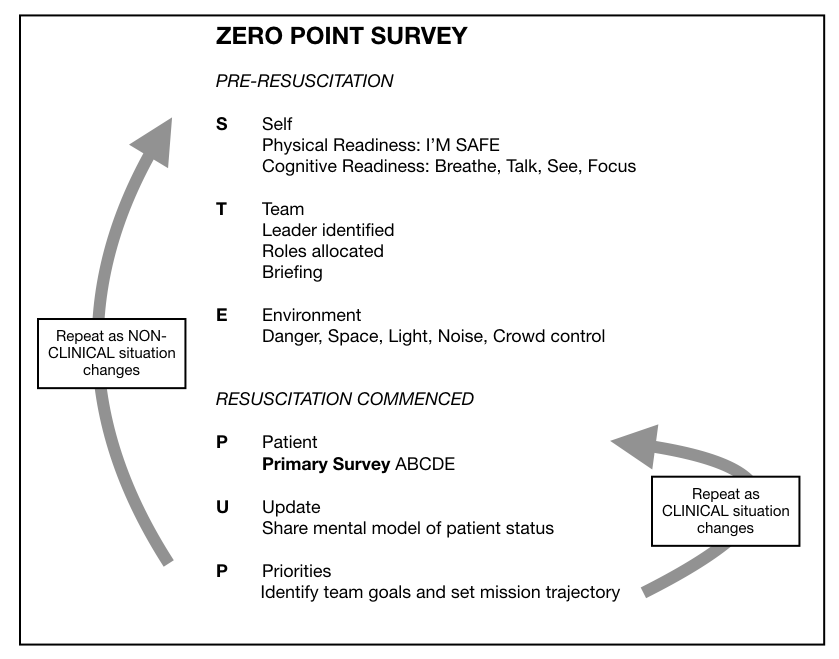
I, along with an international, interdisciplinary faculty of resuscitationists, have previously proposed an easily remembered system for optimising the clinical and non-technical components of resuscitation immediately before and during a patient encounter, dubbed the ‘Zero Point Survey’ (ZPS)(1), so called because first contact with a patient is rarely ‘Time Zero’ for a prehospital mission or hospital resuscitation case; there is invariably time for preparation of oneself, one’s team, and the environment (including equipment) prior to the primary survey and commencement of resuscitation. Following the assessment and management of STEP (self, team, environment & patient), the team should be regularly Updated on patient status and informed of the Priorities.
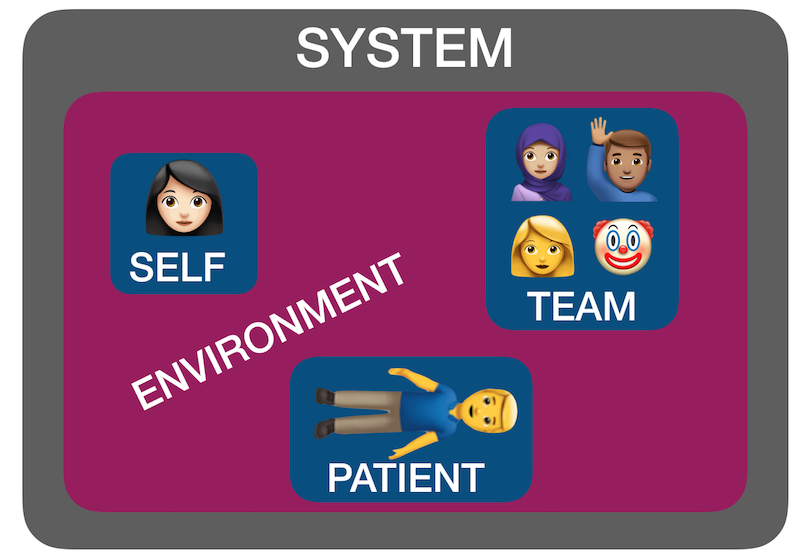
But ‘self, team, environment and patient’ isn’t just a useful system for case preparation. It can also be used for case analysis. I have found by discussing many ‘unsatisfactory’ cases over the years with participants in human factors workshops that STEP can help us identify where the issues lie. Accompanying all these factors is another ’S’: the system in which they interplay – the organisational rules, processes, policies, resources and deficiencies that may facilitate or obstruct an effective resuscitation(2).
Using STEPS to analyse cases The following (genuinely) hypothetical resus cases demonstrate how the application of this framework – Self, Team, Environment, Patient, System – might help identify correctible factors for future resuscitations:
1. Cardiac arrest in the bathroom on the orthopaedic ward – “it was chaos, there were too many people, and the resus trolley wasn’t properly stocked”.
STEPS analysis: Team – Leader needed to assign roles and allocate tasks Environment – Crowd control needed, lack of equipment System – Adequate checks for resus trolley not in place
2. 19-year-old male stabbed in the chest and arrested on arrival in hospital. CPR provided but went from PEA to asystole. Team leader discontinued resus after 20 minutes. Resident: “I thought he needed a resuscitative thoracotomy but no-one was willing to do it. No-one even mentioned it”.
STEPS analysis: Self – Lacked confidence to speak up, doubted own knowledge or influence Team – Lack of team situational awareness or knowledge or skill regarding required intervention System – Insufficient training and preparation for penetrating traumatic cardiac arrest scenario
3. 30-year-old mother with abdominal wound and her 2-year-old daughter with massive open head injury, both due to gunshot wounds, having been shot by husband/father who killed himself on scene. Child arrests in the ED, without ROSC, witnessed by mother before mother is taken to operating theatre.
STEPS analysis: Patient(s) – tragic case with upsetting circumstances and compounded psychological distress for patient and staff. The best resuscitation team in the world is not going to feel good about this one.
4. 46-year-old previously healthy male with VF arrest achieved ROSC after prehospital defibrillation and brought to the ED of a non-cardiac centre comatose and intubated. Further refractory VF in ED. Received multiple shocks, antiarrhythmics, double sequential external defibrillation. No on-site access to mechanical CPR, cardiac catheterisation, or ECMO. Patient declared dead in ED.
STEPS analysis: System – Prehospital team gave excellent care but brought the patient to a hospital ill-equipped to manage his ongoing needs, due to lack of ambulance service policy regarding appropriate destination hospital for cardiac arrest cases.
Summary You can see from the above cases how STEPS may be applied to make some sense of where a resus has gone wrong. Note that I am not recommending this as a way of structuring a team debrief or formal incident investigation – many institutions already have processes for conducting these and various rules and sensitivities have to be accommodated. Rather, this is a format I’ve found helpful in applying during informal discussions that aim to get the nub of where things could or should have gone better.
Occasionally, you can get a case where the STEPS seem to be aligned but things still feel bad – in which the outcome was unsatisfactory because the plan was wrong, or the team wasn’t able to execute the plan. In my next post I’ll discuss another way of analysing cases that can accompany STEPS.
I find clinicians are quick to consider sepsis and hypoperfusion/ischaemia as causes of a raised lactate, but slow to include other causes in their differential.
Although an elevated lactate has been shown to be associated with worse outcomes in numerous studies, not all causes of a raised lactate are sinister. It’s therefore important to diagnose the cause both to allow the right treatment and to avoid assuming an inappropriately poor prognosis.
This 12 minute video offers an approach to diagnosing the cause of elevated lactate based on an understanding of lactate physiology using a simple visual aid – a ‘lactate map’ and a memorable acronym.
Reference
1. Reid C, Rees V, Collyer-Merritt H. Non-septic hyperlactataemia in the emergency department. Emerg Med J. 2010 May;27(5):411–2
This is a guest post from Dr Per Bredmose, anaesthetist and retrieval medicine physician in Norway, also known as Viking One
I struggle to ventilate the patient in the resus room, airway pressures are high, the bag doesn’t empty properly. In my mind I plan ahead for the next step. Through my mind goes the thought – is this the one, the one that I cannot ventilate? Statistically it is not likely to be, but I am prepared to add two-person technique, airway adjuncts like nasopharyngeal or oropharyngeal, or supraglottic devices that I use frequently in theatre. I feel confident in the use of these methods, and (in the worst case) in cricothyroidotomy. I have practiced that numerous times on our live-tissue course on anaesthetised pigs. However – before I start any of these actions.. I routinely, almost as a reflex from theatre turn the patient’s head 45 degrees to the left, and then the bag suddenly empties easily – and I can ventilate the patient.
Some people think that time with TIVA in theatre has little value for emergency medicine and advanced prehospital care. I strongly disagree. This is some of the most relevant and valuable time I have for keeping and optimising my practical skills. Bag-valve-mask (BVM) ventilation is an essential core skill for any prehospital provider. In theatre this manoeuvre is well known and frequently practiced. It is my impression that this head rotation is less used, and even maybe less well known outside theatre, and especially in the prehospital field. Therefore this is a reminder of an old technique.
When to do it: When encountering difficulties in conventional BVM ventilation, either when you cannot ventilate or when it’s just difficult to ventilate.
How to do it: Keep a firm one hand grip and gently rotate the head 45 degrees towards the side of the hand with the jaw grip. At the same time, one can try to optimise the one-hand-jaw thrust that goes along with BVM ventilation. Occasionally one needs to extend (dorsiflex) the neck a bit further to fully open the airway. The technique can also be used as a two-person technique, although this is rarely needed.
Opposition: Frequently I hear that I cannot transfer practice from theatre to the prehospital field. Well, this seems to work well in theatre, in ICU and in the field – airways are airways!!
Recently an article in European Journal of Anaesthesiology by Itagaki et al(1) with a cross over design showed an increase in tidal volume when the patients were ventilated in a head rotated position compared to neutral position with the same airway pressure. Their conclusion was as follows: Head rotation of 45° in anaesthetised apnoeic adults significantly increases the efficiency of mask ventilation compared with the neutral head position. Head rotation is an effective alternative to improve mask ventilation if airway obstruction is encountered. Therefore – this is a useful tool that one always should have in the “practical toolbox”. It is not always the solution, but occasionally it saves you (and the patient) a lot of trouble.
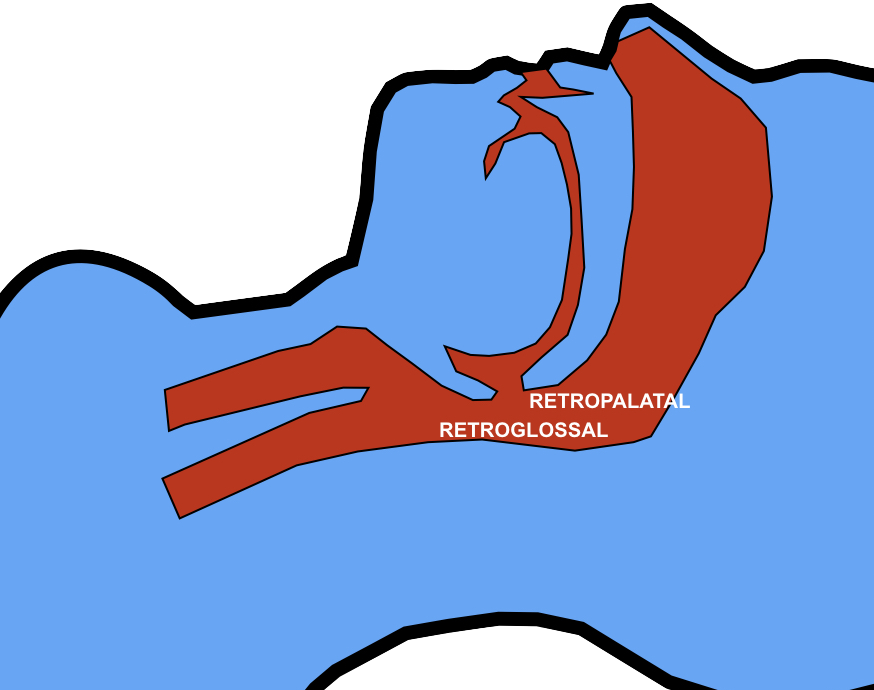
Thoughts from Dr Cliff Reid I haven’t used this approach and wasn’t aware of previous research showing an increase in the retroglossal (but not retropalatine) spaces in (awake) patients with head rotation(2).
The mechanism is thought to be gravitational. It is also possible that neck rotation increases upper airway wall tension that reduces collapsibility of the lumen.
In this elegantly designed new study, a two handed BMV technique was used, similar to that advocated in my prehospital & emergency medicine environments. The rotation was always to the right, although the authors comment that they would expect the same results on the left. The increased tidal volume effect with head rotation occurred mostly in younger patients and patients with Mallampati classification I. Such patients are unlikely to be difficult to mask-ventilate, limiting the applicability of these findings to patients who are difficult to ventilate. However having one more option to employ to improve BMV efficacy (after two person technique, optimising ear-to-sternal-notch positioning, and inserting oro- and/or nasopharyngeal airways) may be useful, and the experience and perspective of my anaesthetic colleague Viking One is definitely food for thought. Obviously one should avoid this if there is potential neck injury so I won’t be trying it my trauma patients.
1. Itagaki T, Oto J, Burns SM, Jiang Y, Kacmarek RM, Mountjoy JR. The effect of head rotation on efficiency of face mask ventilation in anaesthetised apnoeic adults. Eur J Anaesthesiol. 2017 Jul;34(7):432–40.
2. Ono T, Otsuka R, Kuroda T, Honda E, Sasaki T. Effects of head and body position on two- and three-dimensional configurations of the upper airway. J Dent Res. 2000 Nov;79(11):1879–84.
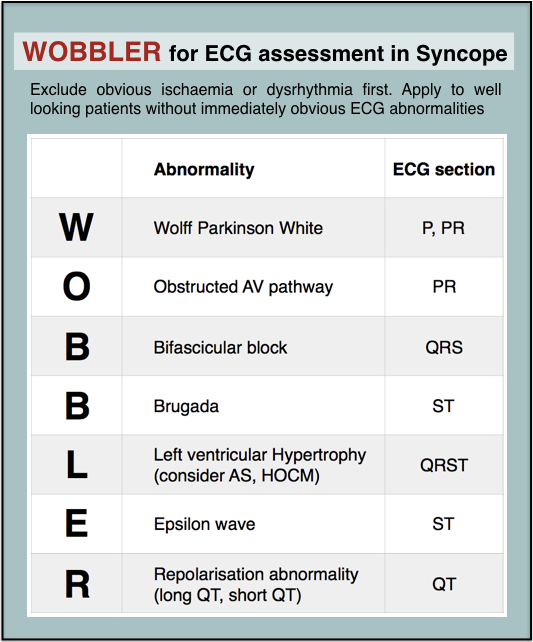
Syncope is a common ED presentation. An ECG is a critical investigation in syncope to identify the cause, including rare conditions associated with risk of sudden cardiac death.
So we should be really grateful when we are invited to interpret an ECG while we’re in the middle of six other tasks.
The problem with syncope is that some of the important life-threatening causes have fairly obscure ECG features that might be hard to remember. Some of these disorders and their ECG features are not entirely familiar to the clinicians who first screen the ECG.
When you’re busy and cognitively stretched you can save time and reduce the risk of missing important findings by having a structured, memorable checklist. I use the acronym WOBBLER, because I don’t want these people to wobble and kiss the dirt again.
The nice thing about WOBBLER is that it uses the sequence that you follow when you look at an ECG, ie from left to right, or from P wave to T wave.
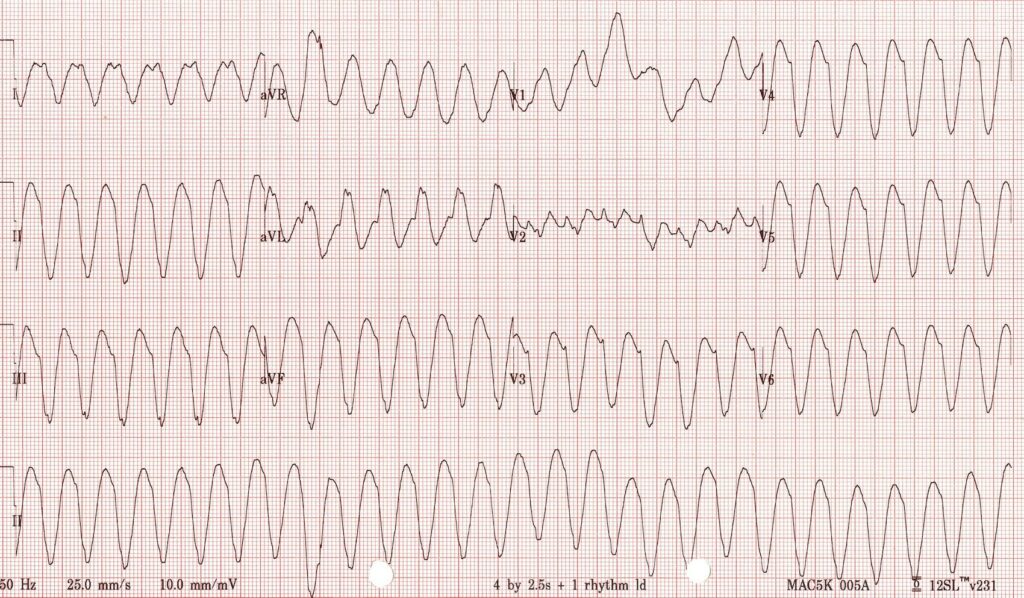
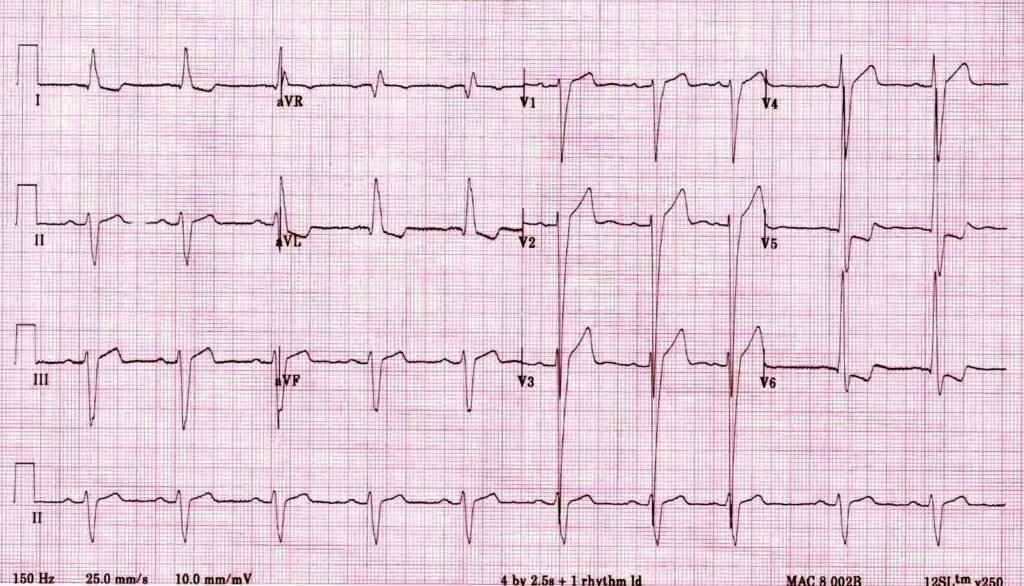
The key is that this is for ECGs without obvious ischaemia or dysrhythmia. If you see something like this (STEMI):
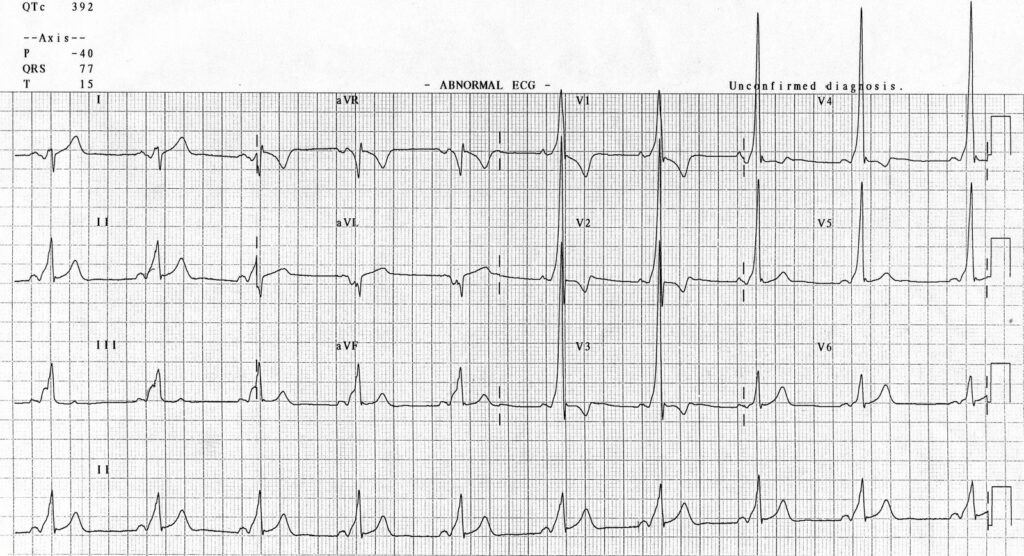
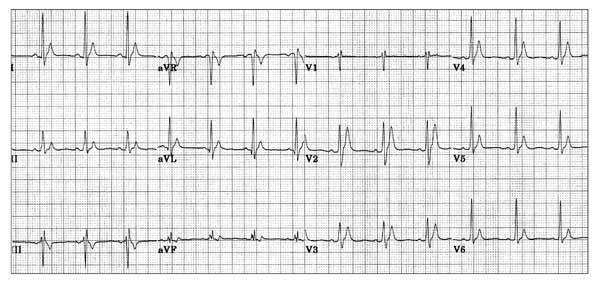
…which is the first step in looking for Bbifascicular block, or the combination of axis deviation and right bundle branch block:
the second B is Brugada, looking for characteristic morphology of the ST segment, so called coved ST elevation:
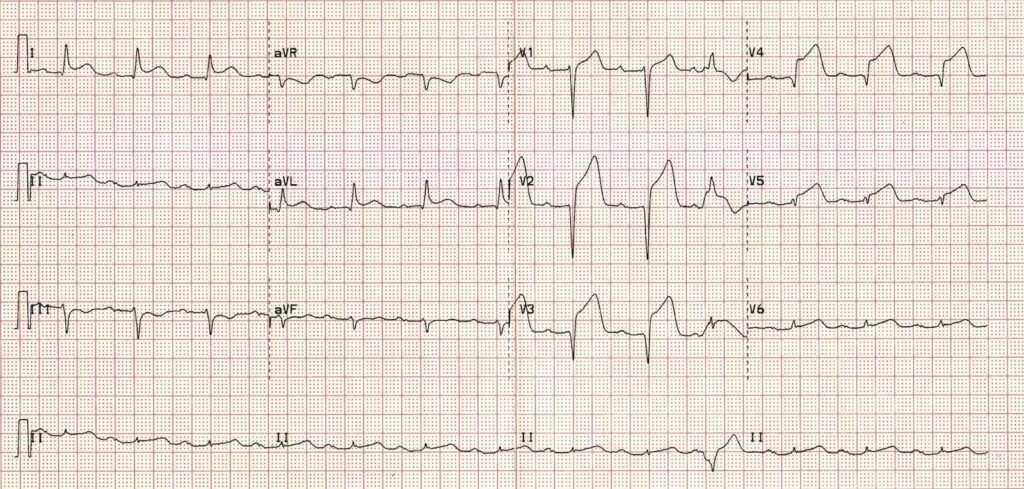
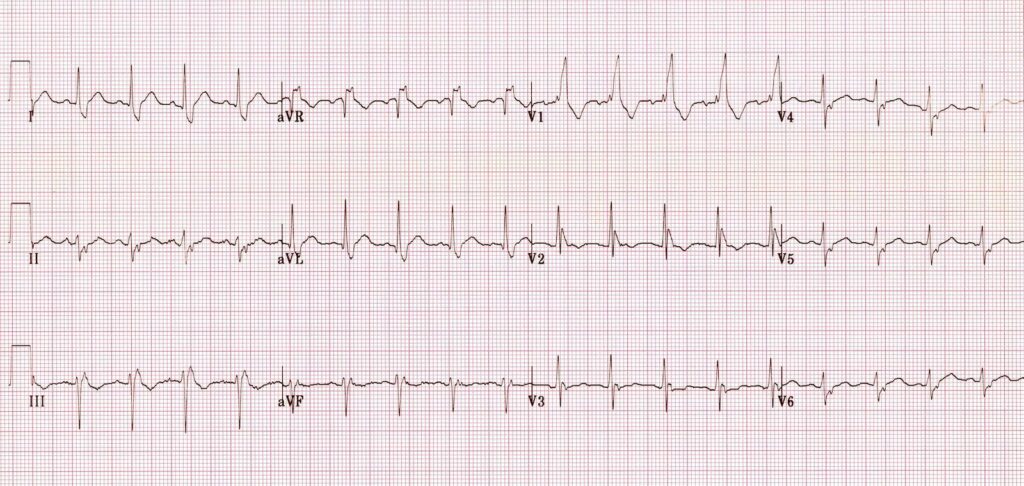
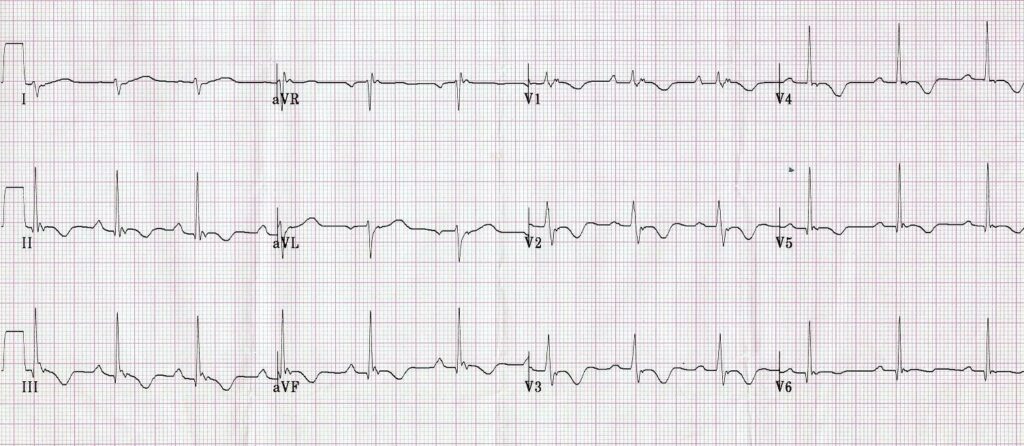
Now syncope, especially exertional syncope, can be caused by left ventricular outflow tract obstruction. Two conditions not to be missed associated with LVOTO (and exertional syncope) are hypertrophic cardiomyopathy and aortic stenosis. These both characteristically cause L– left ventricular hypertrophy:
This example of Hypertrophic Cardiomyopathy has voltage criteria for LVH in the precordial leads as well as narrow, “dagger-like” Q waves in lateral and inferior leads
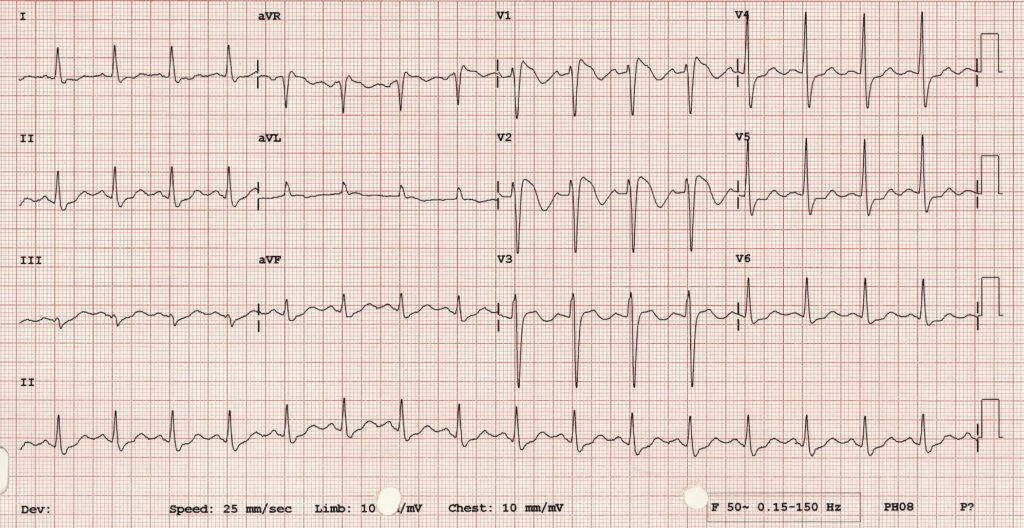
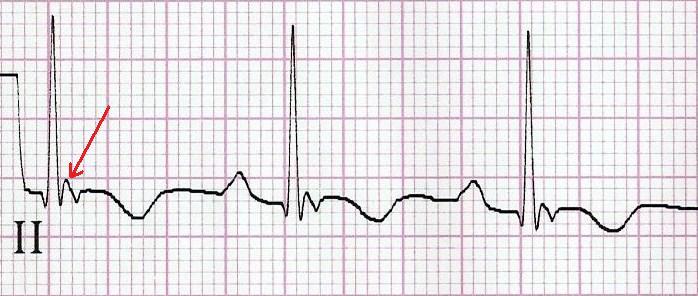
E– stands for epsilon wave, a feature of arrythmogenic right ventricular dysplasia, a rare disorder associated with sudden cardiac death. The epsilon wave looks a bit like the J wave of hypothermia and may be associated with other T wave abnormalities in V1-V3:
Epsilon wave in more detail
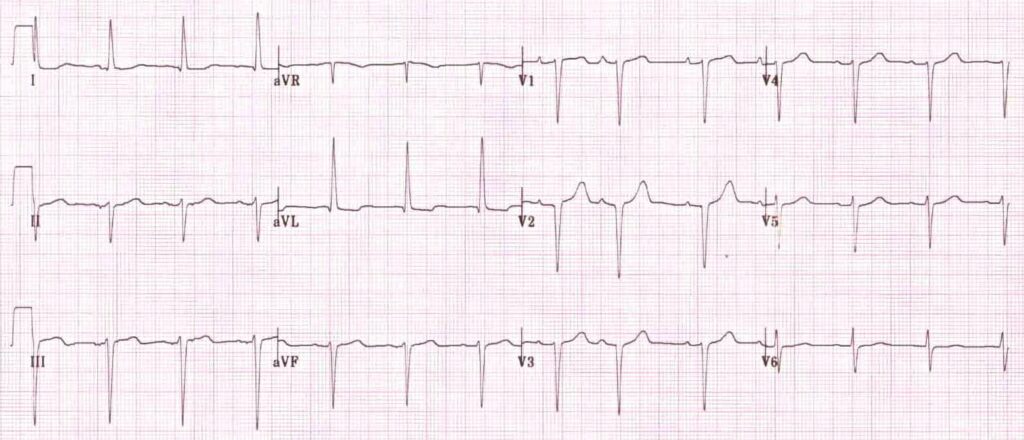
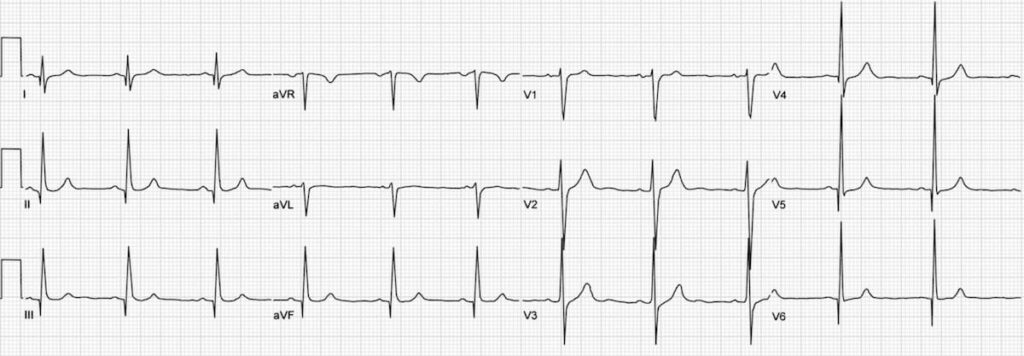
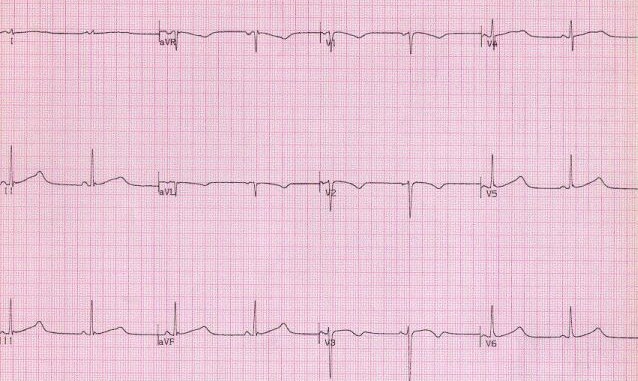
Finally, R stands for Repolarisation abnormality, particularly delayed Repolarisation as found in long QT syndrome:
So WOBBLER may help you find the important and rare abnormalities not to be missed in the syncope patient, going from left to right from P wave through to T wave, in the patient that does not have obvious dysrhythmia or ischaemia. I hope you find it a helpful cognitive forcing tool.
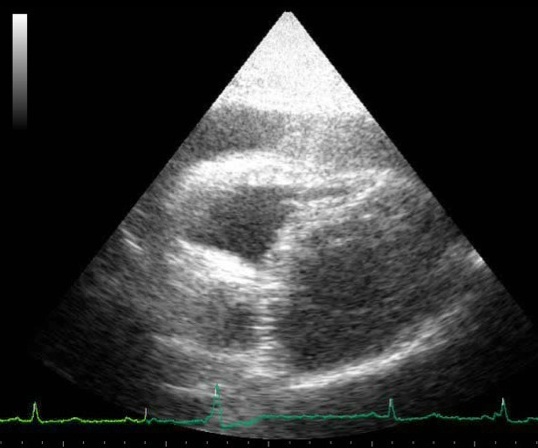
You ultrasound the chest of your shocked patient in resus with fluid refractory hypotension. You see fluid around the heart. The right ventricle keeps bowing inwards, which you recall being described as ‘a little invisible man jumping up and down using the RV as a trampoline’, and you know this is in fact a sign of right ventricular diastolic collapse.
The collapse of the right side of the heart during diastole is the mechanism for shock and cardiac arrest due to tamponade, because the high pericardial pressures prevent the right heart from filling in diastole. This patient therefore has ‘tamponade physiology’ on ultrasound. A quick scan of the IVC shows it is dilated and does not collapse with respiration. This confirms a high central venous pressure (as do the patient’s distended neck veins), also consistent with tamponade physiology.
A formal echo done in resus confirms your suspicion of a dliated aortic root and visible dissection flap, so the diagnosis is now clear. This is type A aortic dissection with tamponade. The patient remains hypotensive and mottled with increasing drowsiness. Cardiothoracic surgery is based at another hospital site 30 minutes away by ambulance.
As the critical care clinician responsible for, or assisting with this patient’s care (emergency physician, intensivist, anaesthetist, rural GP, physician’s assistant, etc.), how do we get this patient to definitive care and mitigate the risk of deterioration en route? Let’s discuss the options using real life case examples, and consider the physiology, the evidence, and the dogma.
Here are four key questions to consider:
1. To drain or not to drain the pericardium?
2. To intubate or not to intubate?
3. If they arrest – CPR or no CPR?
4. How to transfer – physician escort or just send in an ambulance on lights and sirens?
Here are three scenarios that follow the intial assessment of the above patient. They are based on similar cases shared with me by participants on the Critical Care in the Emergency Department course.
Case 1
The patient is obtunded with profound shock and too unstable for transfer. The resus team undertakes pericardiocentesis and aspirates 30 ml of blood. The patient becomes conscious and cooperative and the systolic blood pressure (SBP) is 95 mmHg. The patient is transferred by paramedic ambulance to the cardothoracic centre where he is successfully operated on, resulting in a full recovery.
Case 2
As the patient is unconscious and requires interhospital transfer, the decision is made to intubate him for airway protection. He undergoes rapid sequence induction with ketamine, fentanyl, and rocuronium in the resus room. After capnographic confirmation of tracheal intubation he is manually ventilated via a self-inflating bag. The ED nurse reports a loss of palpable pulse and CPR is started. A team member suggests pericardiocentesis but a senior critical care physician says there is no point because ‘it won’t fix the underlying problem of aortic dissection’ and ’the blood will be clotted anyway’. After a brief attempt at standard ACLS, resuscitation efforts are discontinued and the patient is declared dead.
Case 3
The patient is hypotensive with a SBP of 90mmHg and drowsy but cooperative. The receiving centre has accepted the referral and an ambulance has been requested. The critical care physician responsible for patient transfers is requested to accompany the patient but declines, on the basis that ‘these cases are just like abdominal aortic aneurysms – they just need to get there asap. If they deteriorate en route we’re not going to do anything.’
The patient is transferred but 15 minutes into the journey he becomes unresponsive and loses his cardiac output. The transporting paramedics provide chest compressions and adrenaline/epinephrine but are unable to resuscitate him.
These cases illustrate some of the pitfalls and fallacies associated with tamponade due to type A dissection.
Pericardiocentesis
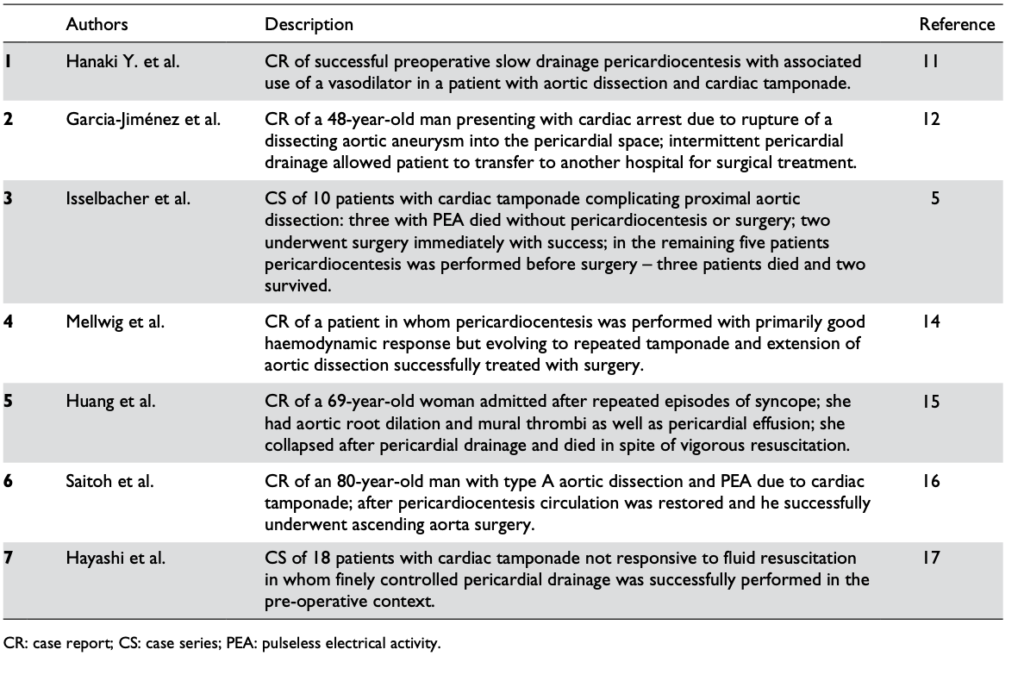
Pericardiocentesis can definitely be life-saving, restoring vital organ perfusion and buying time to get the patient to definitive surgery. Numerous case reports and case series provide evidence of its utility, even in patients in PEA cardiac arrest(1). The authors of the two largest cases series both used 8F pigtail drainage catheters(1,2).
Reports in the literature regarding the pericardiocentesis of critical cardiac tamponade complicating aortic dissection from Cruz et al
One key component of procedural success was controlled pericardial drainage, removing small volumes and reassessing the blood pressure, aiming for a SBP of 90 mmHg. The danger is overshooting, resulting in hypertension and extending the underlying aortic dissection which can be fatal (3).
“In the setting of aortic dissection with haemopericardium and suspicion of cardiac tamponade, emergency transthoracic echocardiography or a CT scan should be performed to confirm the diagnosis. In such a scenario, controlled pericardial drainage of very small amounts of the haemopericardium can be attempted to temporarily stabilize the patient in order to maintain blood pressure at 90 mmHg. (Class IIa, Level C)”
Intubation
Deterioration of tamponade patients following intubation is well described in the literature and the risk is well appreciated by cardiothoracic anaesthetists(5).
Once positive pressure ventilation is started, positive pleural pressure is transmitted to the pericardium, where pressures can exceed right ventricular diastolic pressure and prevent cardiac filling. The result is a fall in and possible loss of cardiac output. This is further exacerbated by the addition of PEEP(6).
One suggested approach if the patient must be intubated for airway protection but is not yet in the operating room with a surgeon ready to cut, is to consider intubation under local anaesthesia and allow the patient to breathe spontaneously (maintaining negative pleural pressure) through the tube until the surgeon is ready to open the chest(5).
Alternatively preload with fluid, use cautious doses of induction agent, and ventilate with low tidal volumes and zero PEEP. However the patient can still crash, so remember that these effects of ventilation on cardiac output in tamponade can be mitigated by the removal of a relatively small volume of pericardial fluid(6).
Cardiac Arrest
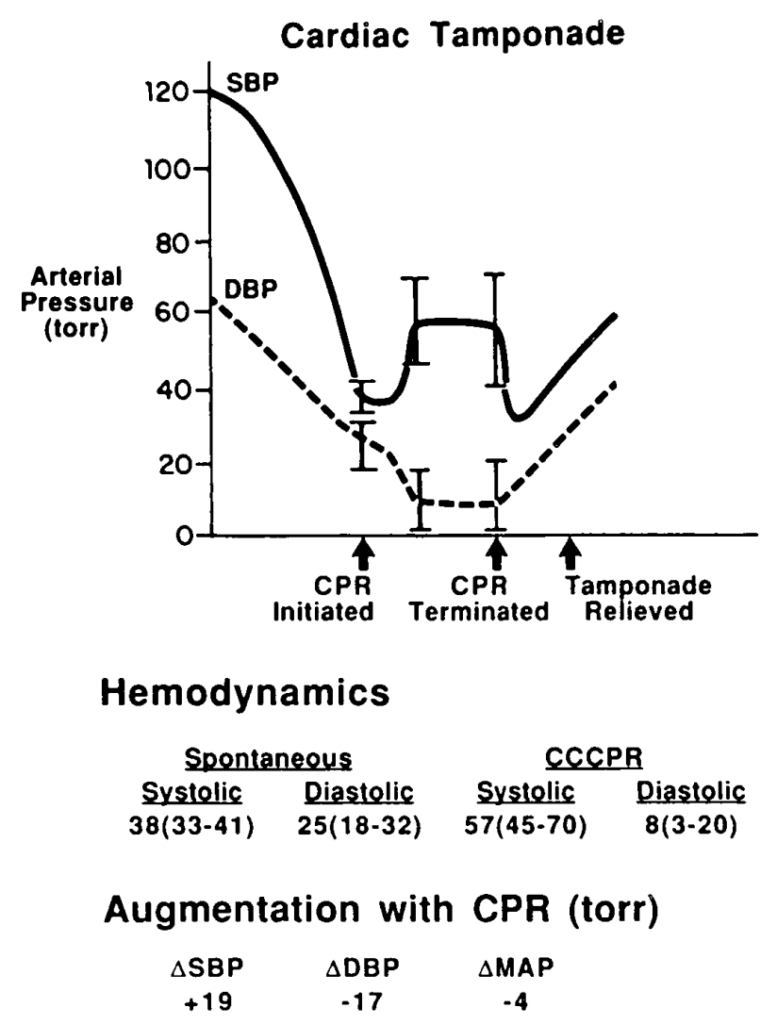
In cardiac arrest, external chest compressions are unlikely to be of benefit. In a study on baboons subjected to cardiac tamponade, closed chest massage resulted in an increase in intrapericardial pressure. There was an increase in systolic pressure, but a marked decrease in diastolic pressure, with an overall decrease in mean arterial pressure(7).
Pressure changes from CPR during tamponade in baboons. From Luna et al (7)
This would lead to impaired coronary perfusion and would be very unlikely to result in return of spontaneous circulation (ROSC). In the clinical situation described above, it is only relief of tamponade that is going to provide an arrested patient with a chance of recovery.
Transport
For patients with cardiac tamponade requiring interhospital (or intrahospital) transfer, it would seem vital therefore that the patient is accompanied by a clinician willing and capable to perform pericardiocentesis in the event of severe deterioriation or arrest en route. This simple life-saving intervention to deliver the patient alive to the operating room should be made available should the need arise.
Summary
Patients presenting in shock from cardiac tamponade often have treatable underlying causes and represent a situation where the planning and actions of the resuscitationist can be truly life-saving.
Pericardiocentesis is recommended in profound shock to buy time for definitive intervention. Controlled pericardiocentesis should be performed paying strict attention to SBP to avoid ‘overshooting’ to a hypertensive state in type A aortic dissection. In cardiac arrest, chest compressions are likely to be ineffective and pericardiocentesis is mandatory for ROSC.
The institution of positive pressure ventilation often results in worsened shock or cardiac arrest, and this is exacerbated by PEEP. Where possible, avoid intubation until the patient is in the operating room, or use low tidal volumes and no PEEP. Even then pericardiocentesis may be necessary to maintain or restore cardiac output.
Patients requiring transport who have tamponade should be accompanied by a clinician able to perform pericardiocentesis in the event of en route deterioration.
References
Cruz I, Stuart B, Caldeira D, Morgado G, Gomes AC, Almeida AR, et al. Controlled pericardiocentesis in patients with cardiac tamponade complicating aortic dissection: Experience of a centre without cardiothoracic surgery. European Heart Journal: Acute Cardiovascular Care. 2015 Mar 19;4(2):124–8.
Hayashi T, Tsukube T, Yamashita T, Haraguchi T, Matsukawa R, Kozawa S, et al. Impact of Controlled Pericardial Drainage on Critical Cardiac Tamponade With Acute Type A Aortic Dissection. Circulation. 2012 Sep 10;126(11_suppl_1):S97–S101.
Isselbacher EM, Cigarroa JE, Eagle KA. Cardiac tamponade complicating proximal aortic dissection. Is pericardiocentesis harmful? Circulation. 1994 Nov 1;90(5):2375–8.
Adler Y, Charron P, Imazio M, Badano L, Barón-Esquivias G, Bogaert J, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. European Heart Journal. 2015 Nov 7;36(42):2921–64.
Ho AMH, Graham CA, Ng CSH, Yeung JHH, Dion PW, Critchley LAH, et al. Timing of tracheal intubation in traumatic cardiac tamponade: A word of caution. Resuscitation. 2009 Feb;80(2):272–4.
Mention the term ‘difficult airway’ and many of us will conjure mental images of some kind of distorted anatomy. However, airway management may be ‘difficult’ for a number of reasons, and no internationally agreed definition of the term exists. Given the wrong staff and circumstances, an ‘easy’ airway in your or my hands may indeed become very difficult. In their editorial “The myth of the difficult airway: airway management revisited” (1) Huitink & Bouwman state:
“In our opinion, the ‘difficult airway’ does not exist. It is a complex situational interplay of patient, practitioner, equipment, expertise and circumstances.”
Airways that are anatomically difficult (eg. limited mouth opening, short thyromental distance, large tongue, neck immobility, etc.) and physiologically difficult (hypoxaemia, hypotension, acidosis) are well described among FOAM resources (2-4). In addition to these, a third category of difficulty is well worth considering.
This last category probably surfaces more commonly than realised, particularly outside the operating room.
Imagine attending a cardiac arrest call on a medical ward. The patient is a 70 year old 120 kg male. The nurses have flattened the bed and discarded the pillow to optimise supine position for CPR. Gobs of vomitus splash from the patient’s pharynx with each compression. The wall suction system is disconnected. There is no bougie in the crash cart’s airway drawer. The nearest capnograph is on another floor of the hospital. In this scenario, no matter how excellent the critical care practitioner’s airway skills, this is a damned difficult airway.
I think Brindley’s third category is a term that should catch on, as a way of helping analyse cases that progress suboptimally and to identify factors during pre-intubation checks that can be addressed. It is terminology that I have added to my own Resuscitese Lexicon, particularly for case discussions during morbidity & mortality and airway audit meetings.
I would like to hear the ‘Situationally Difficult Airway‘ become more widely used, as it fills a gap in how we describe this important area of resuscitation practice.
By Stuart Duffin Expat Brit, intensive care physician and anaesthetist at Karolinska University Hospital in Stockholm, Sweden. Stuart trained in the UK, and spent some time working Australian emergency departments.
One of the most striking things for me about our new/old pan-specialty of critical care, brought into focus by the world-shrinking effects of FOAM and twitter, is just how differently it falls into the domains of the established specialities in different parts of the world. This leads inevitably to comments like, “emergency physicians shouldn’t intubate”, “anaesthetists cant do sick”, “nurses cant be doing such and such”, and so on. All of these statements are clearly equally rubbish because obviously, in certain parts of the world, they do. And they do it really well. Sure there are differences between countries and continents, populations and environments, but when it comes down to it, it doesn’t matter where you are, people still get sick, infected, pregnant, run over, stabbed or hit around the head with heavy things.
All over the world, in our previously quite isolated environments, these same ‘selection pressures’ have forced healthcare providers to evolve by the process of convergent evolution. Although obviously not strictly darwinian, the undeniable effects of simultaneous evolution by survival of the fittest-to-practice can be seen.
Convergent evolution is the process by which, in different parts of the world, completely different species have evolved in parallel to fill similar roles and have similar features. It didn’t matter whether it was a deer, a wildebeest or a kangaroo, there was a vacancy for a fairly big animal who liked eating grass and moved in big groups, and someone stepped up.
Unsurprisingly, critical care resuscitationists are also a little different from country to country and from continent to continent. They have different titles and work in slightly different ways. But when you really look at a critical care doc in action, or talk to one, or follow one on Twitter, we are all cut from the same cloth. I would argue that FOAM has created a critical care zoo in which the kangaroos and antelopes, lemurs and monkeys, aardvarks and echidnas and anaesthetists and emergency physicians are all chucked into the same cage. They’re all looking at each other thinking, “you look like me, but somehow not. We seem to do the same stuff, but we’re not identical – it cant be right!”.
In The United States, the idea of an anaesthetist doing a clamshell thoracotomy would be a little strange. In Scandinavia, an emergency physician doing central lines and fiberoptic intubation in resus would be just as eyebrow raising. A Swedish intensivist and anaesthetist spent some time working in Australia as an ICU senior reg. When attending a patient in resus the emergency physician there announced “we need an airway guy”. My colleague answered “I’m the airway guy”. “No an anaesthetist” replied the emergency physican. “I am an anaesthetist!” “No an….” and so it went on.
The effects of this process are of course by no means limited to doctors. Nurses, paramedics and physiotherapists are all part of this still changing ecosystem. A colleague of mine was showing a visiting Australian emergency physician our trauma bay and describing how major trauma is managed here without the involvement of emergency physicians at all. “When it’s really urgent, it’s anaesthesia and surgery” he explained. I wonder how that went down? There is an element of truth to the statement but the words are wrong. It should have been “When it’s really urgent, it’s airway, access, transfusion, invasive procedures and resuscitation thinking”.
The job title of the person who actually holds the knife/laryngoscope/needle and has what it takes to get it done isn’t important. When the push comes to shove and the bad stuff bounces off the fan, it’s more about skillset and mindset, and less about the collection of letters under your name on your badge, or after your name on your CV.
This talk was the opening plenary given at smacc Chicago. The title they gave me was ‘Advice To A Young Resuscitationist. It’s Up To Us To Save The World‘ but I ditched the last half because, as I point out later in the talk, I don’t think it is up to us to save the whole World. Some AV muppetry at the conference centre prevented the smacc team from being able to include the slides, so I’ll post those too at some point. You can hear the talk as a podcast at the ICN or on iTunes