A study of nonshockable out of hospital cardiac arrest survival showed significant improvement in short- and long-term survival and neurological outcome after implementation of a protocol consistent with CPR guidelines that prioritised chest compressions. These improvements were especially evident among arrests attributable to a cardiac cause, although there was no evidence of harm among arrests attributable to a noncardiac cause.
This was not a randomised trial so unrecognised factors may have contributed to the improved outcome in addition to the change in CPR protocol. However, it is interesting as it provides up to date survival rates from a large population sample: Non shockable out of hospital cardiac arrests achieve return of spontaneous circulation in 34%, 6.8% are discharged from hospital (5.1% with a favourable neurological outcome), and 4.9% survived one year.
The breakdown between PEA and asystole is of course telling, and unsurprising, with 12.8% versus 1.1% being discharged with a favourable neurological outcome, respectively. I would imagine then that some of the PEA patients had beating hearts with hypotension extreme enough to cause pulselessness (pseudo-electromechanical dissociation) – clinically a ‘cardiac arrest’ but really nothing of the sort, and the reason we use cardiac ultrasound to prognosticate.
BACKGROUND: Out-of-hospital cardiac arrest (OHCA) claims millions of lives worldwide each year. OHCA survival from shockable arrhythmias (ventricular fibrillation/ tachycardia) improved in several communities after implementation of American Heart Association resuscitation guidelines that eliminated “stacked” shocks and emphasized chest compressions. “Nonshockable” rhythms are now the predominant presentation of OHCA; the benefit of such treatments on nonshockable rhythms is uncertain.
METHODS AND RESULTS: We studied 3960 patients with nontraumatic OHCA from nonshockable initial rhythms treated by prehospital providers in King County, Washington, over a 10-year period. Outcomes during a 5-year intervention period after adoption of new resuscitation guidelines were compared with the previous 5-year historical control period. The primary outcome was 1-year survival. Patient demographics and resuscitation characteristics were similar between the control (n=1774) and intervention (n=2186) groups, among whom 471 of 1774 patients (27%) versus 742 of 2186 patients (34%), respectively, achieved return of spontaneous circulation; 82 (4.6%) versus 149 (6.8%) were discharged from hospital, 60 (3.4%) versus 112 (5.1%) with favorable neurological outcome; 73 (4.1%) versus 135 (6.2%) survived 1 month; and 48 (2.7%) versus 106 patients (4.9%) survived 1 year (all P≤0.005). After adjustment for potential confounders, the intervention period was associated with an improved odds of 1.50 (95% confidence interval, 1.29-1.74) for return of spontaneous circulation, 1.53 (95% confidence interval, 1.14-2.05) for hospital survival, 1.56 (95% confidence interval, 1.11-2.18) for favorable neurological status, 1.54 (95% confidence interval, 1.14-2.10) for 1-month survival, and 1.85 (95% confidence interval, 1.29-2.66) for 1-year survival.
CONCLUSION: Outcomes from OHCA resulting from nonshockable rhythms, although poor by comparison with shockable rhythm presentations, improved significantly after implementation of resuscitation guideline changes, suggesting their potential to benefit all presentations of OHCA.
Impact of changes in resuscitation practice on survival and neurological outcome after out-of-hospital cardiac arrest resulting from nonshockable arrhythmia Circulation. 2012 Apr 10;125(14):1787-94
A case is reported in Prehospital Emergency Care1 in which an agitated patient (due to mania and alcohol intoxication) received 5 mg/kg (500 mg) of ketamine intramuscularly by an EMS crew which dissociated him within a few minutes. He subsequently developed episodes of laryngospasm in the emergency department which were unrelieved by head tilt, chin lift and simple airway adjuncts but responded to bag-mask ventilation (BMV). The patient was intubated because the laryngospasm recurred, although it had again responded to BMV.
The authors make the point that because of the response of laryngospasm to simple manoeuvres, and because in the prehospital environment a patient will not be left without an EMS provider present, ‘restricting ketamine to EMS units capable of rapid-sequence intubation therefore seems unnecessary.‘
This is one for EMS directors to consider seriously. Personally, I think practicing prehospital care without access to ketamine is like having a hand tied behind my back. Ketamine opens up a world of possibilities in controlling combative patients, optimising scene safety, providing sedation for painful procedures including extrication, and enabling severe pain to be controlled definitively.
I’ve been using ketamine regularly for prehospital analgesia and emergency department procedural sedation in both adults and kids for more than a decade. I’ve seen significant laryngospasm 5 times (twice in kids). On one of those occasions, a 3 year old child desaturated to around 50% twice during two episodes of laryngospasm. We weren’t slow to pick it up – that was just her showing us how quickly kids can desaturate which continued while we went through a stepwise approach until BMV resolved it. It was however an eye opener for the registrar (senior resident) assisting me, who became extremely respectful of ketamine after that. Our ED sedation policy (that I wrote) required that suxamethonium was ready and available and that an appropriate dose had been calculated before anyone got ketamine. Paralysis may extremely rarely be required, but when it’s needed you need to be ready.
The best monitor for laryngospasm – noninvasive capnography
Laryngospasm is rare but most regular prescribers of ketamine will have seen it; the literature says it occurs in about 1-2% of sedations, although anecdotally I think it’s a bit less frequent. Importantly for those weighing the risks of allowing non-RSI competent prescribers, the requirement for intubation is exceptionally rare (2 of 11,589 reported cases in one review). Anyone interested should read this excellent review of ketamine-related adverse effects provided by Chris Nickson at Life in The Fast Lane. Chris reminds us of the Larson manouevre, which is digital pressure in the notch behind and below the ear, described by Larson2 as follows:
The technique involves placing the middle finger of each hand in what I term the laryngospasm notch. This notch is behind the lobule of the pinna of each ear. It is bounded anteriorly by the ascending ramus of the mandible adjacent to the condyle, posteriorly by the mastoid process of the temporal bone, and cephalad by the base of the skull. The therapist presses very firmly inward toward the base of the skull with both fingers, while at the same time lifting the mandible at a right angle to the plane of the body (i.e., forward displacement of the mandible or “jaw thrust”). Properly performed, it will convert laryngospasm within one or two breaths to laryngeal stridor and in another few breaths to unobstructed respirations.
I use this point most often to provide painful stimuli when assessing GCS in a patient, particular those I think may be feigning unconsciousness (I’ve done this for a number of years since learning how painful it can be when I was shown it by a jujitsu instructor). Dr Larson says he was taught the technique by Dr Guadagni, so perhaps we should be calling it the ‘Guadagni manouevre’. The lack of published evidence has led to some appropriate skepticism3, but as it can be combined with a jaw thrust it needn’t delay more aggressive interventions should they become necessary, it may work, and it’s likely to be harmless.
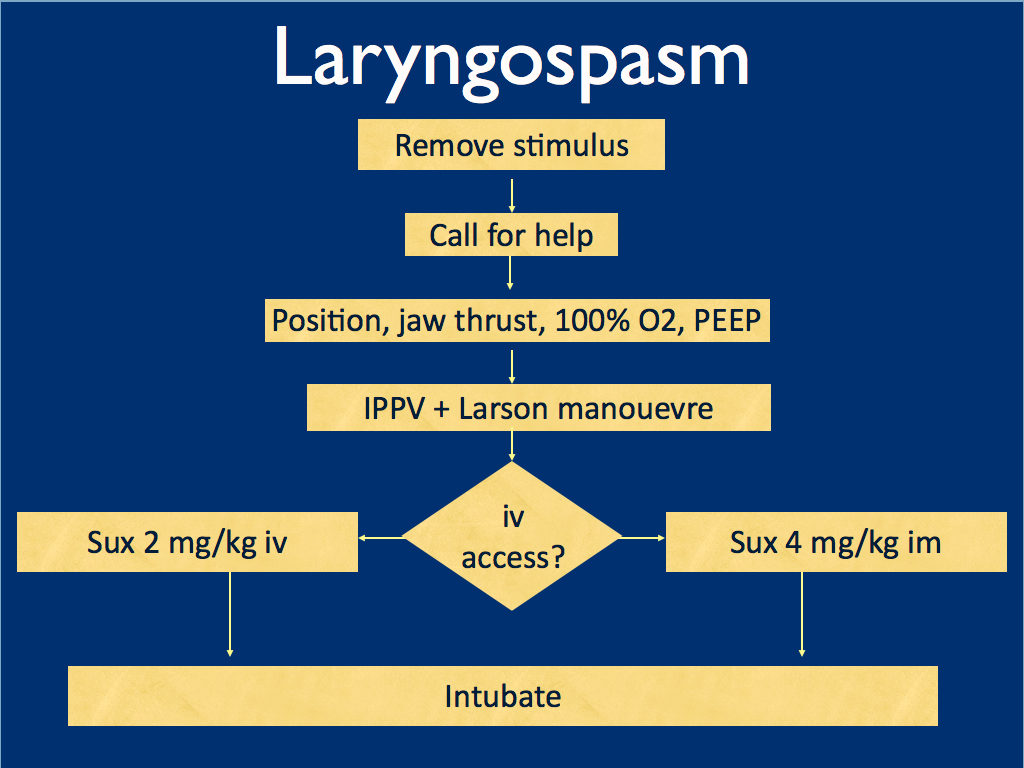
I presented the following suggested algorithm for management of laryngospasm during ketamine procedural sedation at a regional emergency medicine ‘Fellows Forum’ meeting in November 2007 in the UK. Since many paediatric procedural sedations were done using intramuscular (im) ketamine, it gives guidance based on whether or not vascular access has been obtained:
Some things I considered were:
Neuromuscular blockade (NMB) isn’t always necessary – laryngospasm may be managed with other sedatives such as propofol. However, titrating further sedatives in a desaturating child in my view is inferior to definitive airway management and laryngeal relaxation with suxamethonium and a tube.
Laryngospasm may be managed with much smaller doses of suxamethonium than are required for intubation – as little as 0.1 mg/kg may be effective. However, I think once we go down the NMB route we’re committed to intubation and therefore we should use a dose guaranteed to be effective in achieving intubating conditions.
In the child without vascular access, I considered intraosseous and intralingual sux. However, intramuscular suxamethonium is likely to have a relaxant effect on the laryngeal muscles within 30-45 seconds, which has to be compared with time taken to insert and confirm intraosseous needle placement. I do not think the traditionally recommended intralingual injection has any role to play in modern airway management.
At the time I wrote this most paediatric resuscitation bays in my area in the United Kingdom had breathing circuits capable of delivering PEEP – usually the Ayr’s T-Piece (specifically the Mapleson F system), which is why PEEP was included early in in the algorithm prior to BMV.
I have since modified it for two reasons: firstly, we might as well do the Larson manoeuvre during the jaw thrust; secondly, many Australasian and US EDs will only be able to deliver PEEP with a PEEP valve attached to a BVM, so PEEP has been moved to the BVM stage.
I would love to hear what people are doing in their prehospital and inhospital practice. Should ketamine only be administered by providers who can offer RSI? Do you have a laryngospasm protocol? If so, I’d love to see it. If not, feel free to use or adapt my unvalidated one at your own risk.
ABSTRACT An advanced life support emergency medical services (EMS) unit was dispatched with law enforcement to a report of a male patient with a possible overdose and psychiatric emergency. Police restrained the patient and cleared EMS into the scene. The patient was identified as having excited delirium, and ketamine was administered intramuscularly. Sedation was achieved and the patient was transported to the closest hospital. While in the emergency department, the patient developed laryngospasm and hypoxia. The airway obstruction was overcome with bag–valve–mask ventilation. Several minutes later, a second episode of laryngospasm occurred, which again responded to positive-pressure ventilation. At this point the airway was secured with an endotracheal tube. The patient was uneventfully extubated several hours later. This is the first report of laryngospam and hypoxia associated with prehospital administration of intramuscular ketamine to a patient with excited delirium.
A military study revealed troops suffering from severe burns tended to receive either no prehospital fluid or too much fluid1.
The authors point out some practical realities and an attempted solution:
For a medic potentially treating multiple casualties at once in a hostile environment, the calculation of the modified Brooke or Parkland formula may be unrealistic prior to beginning fluid resuscitation in the prehospital setting.
The USAISR’s Rule of 10 is a simplified formula to guide the initial fluid resuscitation of a burn victim. The burn size is estimated to the nearest 10% TBSA. For patients weighing 40 to 80 kg, the burn size is then multiplied by 10 to give the initial fluid rate in milliliters per hour. The rate is increased by 100 mL/hour for every 10 kg above 80 kg in terms of the patient’s weight. For the majority of adult burn patients, the Rule of 10 approximates the initial fluid rate within accepted ABA guidelines.
A previous study on the rule of 10 showed it provided an estimate that fell between the modified Brooke and Parkland estimates 87.8% of the time, less than the modified Brooke <12% of the time, and hardly ever (>1%) exceeded the Parkland estimate2.
OBJECTIVE: The purpose of this article is to provide a descriptive study of the management of burns in the prehospital setting of a combat zone.
METHODS: A retrospective chart review was performed of U.S. casualties with >20% total-body-surface-area thermal burns, transported from the site of injury to Ibn Sina Combat Support Hospital (CSH) between January 1, 2006, and August 30, 2009.
RESULTS: Ibn Sina CSH received 225 burn casualties between January 2006 and August 2009. Of these, 48 met the inclusion criteria. The mean Injury Severity Score was 31.7 (range 4 to 75). Prehospital vascular access was obtained in 24 casualties (50%), and 20 of the casualties received fluid resuscitation. Out of the 48 casualties enrolled, 28 (58.3%) did not receive prehospital fluid resuscitation. Of the casualties who received fluid resuscitation, nearly all received volumes in excess of the guidelines established by the American Burn Association and those recommended by the Committee for Tactical Combat Casualty Care. With regard to pain management in the prehospital setting, 13 casualties (27.1%) received pain medication.
CONCLUSIONS: With regard to the prehospital fluid resuscitation of primary thermal injury in the combat zone, two extremes were noted. The first group did not receive any fluid resuscitation; the second group was resuscitated with fluid volumes higher than those expected if established guidelines were utilized. Pain management was not uniformly provided to major burn casualties, even in several with vascular access. These observations support improved education of prehospital personnel serving in a combat zone.
Tracheal extubation is a high risk procedure in anaesthesia and critical care. Until now most guidelines have focused on intubation, with little to guide the process of extubation. Complications may relate to the following issues:
Exaggerated reflexes – laryngospasm (which can lead to both hypoxia and negative pressure pulmonary oedema) and bronchospasm
Reduced airway reflexes
Dysfunctional laryngeal reflexes
Depletion of oxygen stores at extubation
Airway injury
Physiological compromise in other systems
Human factors
The goal is to ensure uninterrupted oxygen delivery to the patient’s lungs, avoid airway stimulation, and have a back-up plan, that would permit ventilation and re-intubation with minimum difficulty and delay should extubation fail.
The Difficult Airway Society has now published guidelines for the management of tracheal extubation, describing four steps:
Step 1: plan extubation.
Step 2: prepare for extubation.
Step 3: perform extubation.
Step 4: post-extubation care: recovery and follow-up.
During step 3, emphasis is on pre-oxygenation, positioning, and suction. This is followed by simultaneous deflation of the tracheal tube cuff and removal of the tube at the peak of a sustained inflation. This generates a passive exhalation, which may assist in the expulsion of secretions and possibly reduce the incidence of laryngospasm and breathholding.
The guideline refers to low-risk and at-risk extubations. ‘Low-risk’ (routine) extubation is characterised by the expectation that reintubation could be managed without difficulty, if required. ‘At-risk’ means the presence of general and/or airway risk factors that suggest that a patient may not be able to maintain his/her own airway after removal of the tracheal tube. ‘At-risk’ extubation is characterised by the concern that airway management may not be straightforward should reintubation be required.
These guidelines are written for the peri-operative patient but the text contains some interesting points that are pertinent to the ED or ICU patient. Some simple algorithms are presented:
A multidisciplinary panel of 28 experts from eight countries reviewed the literature and came up with consensus guidelines in point-of-care lung ultrasound. There were some big names involved – all the big players in emergency/critical care ultrasound from around the World. Conspicuously absent were Matt and Mike from the Emergency Ultrasound Podcast, but maybe there was a maximum awesomeness limit or something.
Here are some snippets, taken out of context and without the grade of recommendation attached. Try to get hold of the original if you can, which might not be easy. I never understand it when ‘international recommendations’ are published as subscription-only articles. Either they want people to follow them or not. Oh well – here are some of their recommendations: Pneumothorax
The sonographic signs of pneumothorax include the following: Presence of lung point(s); Absence of lung sliding; Absence of B-lines; Absence of lung pulse
The lung pulse refers to the subtle rhythmic movement of the visceral upon the parietal pleura with cardiac oscillations and is a rule-out sign for pneumothorax
In the supine patient, the sonographic technique consists of exploration of the least gravitationally dependent areas progressing more laterally.
Bedside lung ultrasound is a useful tool to differentiate between small and large pneumothorax, using detection of the lung point.
Interstitial syndrome
B-lines are defined as discrete laser-like vertical hyperechoic reverberation artifacts that arise from the pleural line (previously described as ‘‘comet tails’’), extend to the bottom of the screen without fading, and move synchronously with lung sliding.
The presence of multiple diffuse bilateral B-lines indicates interstitial syndrome. Causes of interstitial syndrome include the following conditions: Pulmonary edema of various causes; Interstitial pneumonia or pneumonitis; Diffuse parenchymal lung disease (pulmonary fibrosis)
Lung consolidation
The sonographic sign of lung consolidation is a subpleural echo-poor region or one with tissue-like echotexture.
Lung ultrasound is a clinically useful tool to rule in pneumonia; however, lung ultrasound does not rule out consolidations that do not reach the pleura.
In mechanically ventilated patients lung ultrasound should be considered as it is more accurate than portable chest radiography in the detection of consolidation.
Pleural effusion
Both of the following signs are present in almost all free effusions: A space (usually anechoic) between the parietal and visceral pleura; Respiratory movement of the lung within the effusion (‘‘sinusoid sign’’)
In opacities identified by chest radiography, lung ultrasound should be used because it is more accurate than chest radiography in distinguishing between effusion and consolidation.
Visualization of internal echoes, either of mobile particles or septa, is highly suggestive of exudate or hemothorax
BACKGROUND: The purpose of this study is to provide evidence-based and expert consensus recommendations for lung ultrasound with focus on emergency and critical care settings.
METHODS: A multidisciplinary panel of 28 experts from eight countries was involved. Literature was reviewed from January 1966 to June 2011. Consensus members searched multiple databases including Pubmed, Medline, OVID, Embase, and others. The process used to develop these evidence-based recommendations involved two phases: determining the level of quality of evidence and developing the recommendation. The quality of evidence is assessed by the grading of recommendation, assessment, development, and evaluation (GRADE) method. However, the GRADE system does not enforce a specific method on how the panel should reach decisions during the consensus process. Our methodology committee decided to utilize the RAND appropriateness method for panel judgment and decisions/consensus.
RESULTS: Seventy-three proposed statements were examined and discussed in three conferences held in Bologna, Pisa, and Rome. Each conference included two rounds of face-to-face modified Delphi technique. Anonymous panel voting followed each round. The panel did not reach an agreement and therefore did not adopt any recommendations for six statements. Weak/conditional recommendations were made for 2 statements, and strong recommendations were made for the remaining 65 statements. The statements were then recategorized and grouped to their current format. Internal and external peer-review processes took place before submission of the recommendations. Updates will occur at least every 4 years or whenever significant major changes in evidence appear.
CONCLUSIONS: This document reflects the overall results of the first consensus conference on “point-of-care” lung ultrasound. Statements were discussed and elaborated by experts who published the vast majority of papers on clinical use of lung ultrasound in the last 20 years. Recommendations were produced to guide implementation, development, and standardization of lung ultrasound in all relevant settings.
‘You can’t clear the cervical spine until the patient wakes up!’ How often have you heard this said about a patient with severe traumatic brain injury who may not ‘wake up’ for weeks, if at all?
A controversial area, but many institutions now allow collar removal if a neck CT scan is normal. Does this rule out injury with 100% sensitivity? No – but it probably pushes the balance of risk towards removing the collar – an intervention with no evidence for benefit and plenty of reasons why it may be harmful to ventilated ICU patients. For example, clearing the cervical spine based on MDCT was associated with less delirium and less ventilator associated pneumonia, both of which have been associated with increased mortality in critically ill patients (this is referenced in the paper below).
The UK’s Intensive Care Society has had pragmatic guidelines along these lines since 2005, which can be found here. This month’s Intensive Care Medicine publishes an updated literature review providing some further support to this approach.
PURPOSE: Controversy exists over how to ‘clear’ (we mean enable the clinician to safely remove spinal precautions based on imaging and/or clinical examination) the spine of significant unstable injury among clinically unevaluable obtunded blunt trauma patients (OBTPs). This review provides a clinically relevant update of the available evidence since our last review and practice recommendations in 2004.
METHODS: Medline, Embase. Google Scholar, BestBETs, the trip database, BMJ clinical evidence and the Cochrane library were searched. Bibliographies of relevant studies were reviewed.
RESULTS: Plain radiography has low sensitivity for detecting unstable spinal injuries in OBTPs whereas multidetector-row computerised tomography (MDCT) approaches 100%. Magnetic resonance imaging (MRI) is inferior to MDCT for detecting bony injury but superior for detecting soft tissue injury with a sensitivity approaching 100%, although 40% of such injuries may be stable and ‘false positive’. For studies comparing MDCT with MRI for OBTPs; MRI following ‘normal’ CT may detect up to 7.5% missed injuries with an operative fixation in 0.29% and prolonged collar application in 4.3%. Increasing data is available on the complications associated with prolonged spinal immobilisation among a population where a minority have an actual injury.
CONCLUSIONS: Given the variability of screening performance it remains acceptable for clinicians to clear the spine of OBTPs using MDCT alone or MDCT followed by MRI, with implications to either approach. Ongoing research is needed and suggestions are made regarding this. It is essential clinicians and institutions audit their data to determine their likely screening performances in practice.
The prevention and management of venous thromboembolic disease is a huge topic, which generates questions for emergency, critical care, and acute physicians during many shifts:
How long should someone requiring cardioversion for atrial fibrillation be anticoagulated for?
How should I provide thromboprophylaxis for this intubated patient?
This patient with submassive pulmonary embolism isn’t hypotensive yet. Can I thrombolyse them? Can I?
There’s a large superficial vein thrombosis in that limb – is anticoagulation indicated?
This asymptomatic patient on warfarin has an INR of 9.0 – should I reverse them?
Do I need to add Vitamin K if I’ve reversed warfarin with prothrombin complex concentrate?
The answers to these – and many, many more – questions are provided in one of the most comprehensive guidelines I’ve ever come across. I can see myself clicking on the link below in future when on duty in the ED. Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines Chest. 2012 Feb;141(2 Suppl) Full Text
The European Society of Intensive Care Medicine has produced a consensus statement on colloid volume therapy for critically ill patients, published in this month’s Intensive Care Medicine.
Curiously, the full text document is not yet availablle on ESICM’s website, but I found this presentation summarising the work by one the authors (Richard Beale):
PURPOSE: Colloids are administered to more patients than crystalloids, although recent evidence suggests that colloids may possibly be harmful in some patients. The European Society of Intensive Care Medicine therefore assembled a task force to compile consensus recommendations based on the current best evidence for the safety and efficacy of the currently most frequently used colloids-hydroxyethyl starches (HES), gelatins and human albumin.
METHODS: Meta-analyses, systematic reviews and clinical studies of colloid use were evaluated for the treatment of volume depletion in mixed intensive care unit (ICU), cardiac surgery, head injury, sepsis and organ donor patients. Clinical endpoints included mortality, kidney function and bleeding. The relevance of concentration and dosage was also assessed. Publications from 1960 until May 2011 were included. The quality of available evidence and strength of recommendations were based on the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach.
RECOMMENDATIONS AND CONCLUSIONS: We recommend not to use HES with molecular weight ≥200 kDa and/or degree of substitution >0.4 in patients with severe sepsis or risk of acute kidney injury and suggest not to use 6% HES 130/0.4 or gelatin in these populations. We recommend not to use colloids in patients with head injury and not to administer gelatins and HES in organ donors. We suggest not to use hyperoncotic solutions for fluid resuscitation. We conclude and recommend that any new colloid should be introduced into clinical practice only after its patient-important safety parameters are established.
Consensus statement of the ESICM task force on colloid volume therapy in critically ill patients Intensive Care Med. 2012 Mar;38(3):368-83 Update September 2012:
An RCT showed patients with severe sepsis assigned to fluid resuscitation with HES 130/0.42 had an increased risk of death at day 90 and were more likely to require renal-replacement therapy, as compared with those receiving Ringer’s acetate. Read more about the trial here Hydroxyethyl Starch 130/0.42 versus Ringer’s Acetate in Severe Sepsis N Engl J Med. 2012 Jul 12;367(2):124-34
Australian intensivist John Myburgh gives a great summary of Fluid Therapy in critical care here
A post hoc reanalysis was performed on a 2009 JAMA paper comparing patients randomised to receive or not receive prehospital drugs and iv access for cardiac arrest.
This was done to evaulate the effect of adrenaline/epinephrine. The reason for the reanalysis was that in the original intention-to-treat analysis, some of the following issues may have influenced the results:
Some patients randomised to adrenaline never received it as they had ROSC before the drug could be given, thus yielding a selection bias with the most easily resuscitated patients in the post hoc no-adrenaline group
At least 1 of 5 patients randomised to receive IV access and drugs did not receive adrenaline as it was regarded futile or it was impossible to gain intravenous access
1 of 10 patients randomised to not receive drugs received adrenaline after they had regained spontaneous circulation for > 5 min.
The purpose of this post hoc analysis on the RCT data was to compare outcomes for patients actually receiving adrenaline to those not receiving adrenaline.
The actual use of adrenaline was associated with increased short-term survival, but with 48% less survival to hospital discharge. The improved survival to hospital admission is consistent with the results of a recent Australia study, and the negative association with longer term survival is similar to a multivariate analysis of observational Swedish registry data where patients receiving adrenaline were 57% less likely to be alive after one month.
Yet more evidence that we haven’t found any drugs proven to improve survival in cardiac arrest. At least not until the human studies on sodium nitroprusside come out?
I bet some of you are still going to be giving the epi exactly every four minutes though.
**Update: see Prehospital Epinephrine Use and Survival Among Patients With Out-of-Hospital Cardiac Arrest – more prospective data from Japan, this time showing epinephrine improves prehospital ROSC, but decreases chance of survival and good functional outcomes 1 month after the event.**
PURPOSE OF THE STUDY: IV line insertion and drugs did not affect long-term survival in an out-of-hospital cardiac arrest (OHCA) randomized clinical trial (RCT). In a previous large registry study adrenaline was negatively associated with survival from OHCA. The present post hoc analysis on the RCT data compares outcomes for patients actually receiving adrenaline to those not receiving adrenaline.
MATERIALS AND METHODS: : Patients from a RCT performed May 2003 to April 2008 were included. Three patients from the original intention-to-treat analysis were excluded due to insufficient documentation of adrenaline administration. Quality of cardiopulmonary resuscitation (CPR) and clinical outcomes were compared.
RESULTS: Clinical characteristics were similar and CPR quality comparable and within guideline recommendations for 367 patients receiving adrenaline and 481 patients not receiving adrenaline. Odds ratio (OR) for being admitted to hospital, being discharged from hospital and surviving with favourable neurological outcome for the adrenaline vs. no-adrenaline group was 2.5 (CI 1.9, 3.4), 0.5 (CI 0.3, 0.8) and 0.4 (CI 0.2, 0.7), respectively. Ventricular fibrillation, response interval, witnessed arrest, gender, age and endotracheal intubation were confounders in multivariate logistic regression analysis. OR for survival for adrenaline vs. no-adrenaline adjusted for confounders was 0.52 (95% CI: 0.29, 0.92).
CONCLUSION: Receiving adrenaline was associated with improved short-term survival, but decreased survival to hospital discharge and survival with favourable neurological outcome after OHCA. This post hoc survival analysis is in contrast to the previous intention-to-treat analysis of the same data, but agrees with previous non-randomized registry data. This shows limitations of non-randomized or non-intention-to-treat analyses.
Outcome when adrenaline (epinephrine) was actually given vs. not given – post hoc analysis of a randomized clinical trial Resuscitation. 2012 Mar;83(3):327-32
The Brain Trauma Foundation has released updated guidelines on traumatic brain injury in children.
Most of the recommendations are Grade C and therefore based on limited evidence.
Indications for ICP monitoring
Use of intracranial pressure (ICP) monitoring may be considered in infants and children with severe traumatic brain injury (TBI) (Grade C). Four lines of evidence support the use of ICP monitoring in children with severe TBI:
a frequently reported high incidence of intracranial hypertension in children with severe TBI
a widely reported association of intracranial hypertension and poor neurologic outcome
the concordance of protocol-based intracranial hypertension therapy and best-reported clinical outcomes
and improved outcomes associated with successful ICP-lowering therapies.
Threshold for treatment of intracranial hypertension
Treatment of intracranial pressure (ICP) may be considered at a threshold of 20 mm Hg (Grade C). Sustained elevations in ICP (>20 mm Hg) are associated with poor outcome in children after severe TBI. Normal values of blood pressure and ICP are age-dependent (lower at younger ages), so it is anticipated that the optimal ICP treatment threshold may be age-dependent. Cerebral perfusion pressure thresholds
A CPP threshold 40–50 mm Hg may be considered. There may be age-specific thresholds with infants at the lower end and adolescents at the upper end of this range (Grade C). Survivors of severe pediatric TBI undergoing ICP monitoring consistently have higher CPP values vs. nonsurvivors, but no study demonstrates that active maintenance of CPP above any target threshold in pediatric TBI reduces mortality or morbidity. CPP should be determined in a standard fashion with ICP zeroed to the tragus (as an indicator of the foramen of Monro and midventricular level) and MAP zeroed to the right atrium with the head of the bed elevated 30°. Advanced neuromonitoring
If brain oxygenation monitoring is used, maintenance of partial pressure of brain tissue oxygen (PbtO2) >10 mm Hg may be considered. Neuroimaging
In the absence of neurologic deterioration or increasing intracranial pressure (ICP), obtaining a routine repeat computed tomography (CT) scan >24 hrs after the admission and initial follow-up study may not be indicated for decisions about neurosurgical intervention (Grade C). Hyperosmolar therapy
Hypertonic saline should be considered for the treatment of severe pediatric traumatic brain injury (TBI) associated with intracranial hypertension. Effective doses for acute use range between 6.5 and 10 mL/kg (of 3%) (Grade B). Hypertonic saline should be considered for the treatment of severe pediatric TBI associated with intracranial hypertension. Effective doses as a continuous infusion of 3% saline range between 0.1 and 1.0 mL/kg of body weight per hour administered on a sliding scale. The minimum dose needed to maintain intracranial pressure (ICP) Temperature control
Moderate hypothermia (32–33°C) beginning early after severe traumatic brain injury (TBI) for only 24 hrs’ duration should be avoided.
Moderate hypothermia (32–33°C) be- ginning within 8 hrs after severe TBI for up to 48 hrs’ duration should be considered to reduce intracranial hypertension.
If hypothermia is induced for any indication, rewarming at a rate of >0.5°C/hr should be avoided (Grade B).
Moderate hypothermia (32–33°C) be- ginning early after severe TBI for 48 hrs, duration may be considered (Grade C). Note: after completion of these guidelines, the committee became aware that the Cool Kids trial of hypothermia in pediatric TBI was stopped because of futility. The implications of this development on the recommendations in this section may need to be considered by the treating physician when details of the study are published. Cerebrospinal fluid drainage
Cerebrospinal fluid (CSF) drainage through an external ventricular drain may be considered in the management of increased intracranial pressure (ICP) in children with severe traumatic brain injury (TBI).
The addition of a lumbar drain may be considered in the case of refractory intracranial hypertension with a functioning external ventricular drain, open basal cis- terns, and no evidence of a mass lesion or shift on imaging studies (Grade C). Barbiturates
High-dose barbiturate therapy may be considered in hemodynamically stable patients with refractory intracranial hypertension despite maximal medical and surgical management.
When high-dose barbiturate therapy is used to treat refractory intracranial hy- pertension, continuous arterial blood pressure monitoring and cardiovascular support to maintain adequate cerebral perfusion pressure are required (Grade C). Decompressive craniectomy for the treatment of intracranial hypertension
Decompressive craniectomy (DC) with duraplasty, leaving the bone flap out, may be considered for pediatric patients with traumatic brain injury (TBI) who are showing early signs of neurologic deterioration or herniation or are developing intracranial hypertension refractory to medical management during the early stages of their treatment (Grade C). Hyperventilation
Avoidance of prophylactic severe hyperventilation to a PaCO2 If hyperventilation is used in the management of refractory intracranial hypertension, advanced neuromonitoring for evaluation of cerebral ischemia may be considered (Grade C). Corticosteroids
The use of corticosteroids is not recommended to improve outcome or reduce intracranial pressure (ICP) for children with severe traumatic brain injury (TBI) (Grade B). Analgesics, sedatives, and neuromuscular blockade
Etomidate may be considered to control severe intracranial hypertension; however, the risks resulting from adrenal suppression must be considered.
Thiopental may be considered to control intracranial hypertension.
In the absence of outcome data, the specific indications, choice and dosing of analgesics, sedatives, and neuromuscular-blocking agents used in the management of infants and children with severe traumatic brain injury (TBI) should be left to the treating physician.
*As stated by the Food and Drug Administration, continuous infusion of propofol for either sedation or the management of refractory intracranial hypertension in infants and children with severe TBI is not recommended (Grade C). The availability of other sedatives and analgesics that do not suppress adrenal function, small sample size and single-dose administration in the study discussed previously, and limited safety profile in pediatric TBI limit the ability to endorse the general use of etomidate as a sedative other than as an option for single-dose administration in the setting of raised ICP. Glucose and nutrition
The evidence does not support the use of an immune-modulating diet for the treatment of severe traumatic brain injury (TBI) to improve outcome (Grade B).
In the absence of outcome data, the specific approach to glycemic control in the management of infants and children with severe TBI should be left to the treating physician (Grade C). Antiseizure prophylaxis
Prophylactic treatment with phenytoin may be considered to reduce the incidence of early posttraumatic seizures (PTS) in pediatric patients with severe traumatic brain injury (TBI) (Grade C). The incidence of early PTS in pediatric patients with TBI is approximately 10% given the limitations of the available data. Based on a single class III study (4), prophylactic anticonvulsant therapy with phenytoin may be considered to reduce the incidence of early posttraumatic seizures in pediatric patients with severe TBI. Concomitant monitoring of drug levels is appropriate given the potential alterations in drug metabolism described in the context of TBI. Stronger class II evidence is available supporting the use of prophylactic anticonvulsant treatment to reduce the risk of early PTS in adults. There are no compelling data in the pediatric TBI literature to show that such treatment reduces the long-term risk of PTS or improves long-term neurologic outcome. Guidelines for the Acute Medical Management of Severe Traumatic Brain Injury in Infants, Children, and Adolescents-Second Edition Pediatr Crit Care Med 2012 Vol. 13, No. 1 (Suppl.) Read online Download PDF (617k) Other Brain Trauma Foundation Guidelines